

Acromioclavicular Joint Injuries: Effective Rehabilitation
- PMID: 34093044
- PMCID: PMC8169819
- DOI: 10.2147/OAJSM.S244283
Acromioclavicular Joint Injuries: Effective Rehabilitation
Abstract
Purpose: To perform a review of the literature focusing on rehabilitation protocols in patients with acromioclavicular (AC) joint injuries treated operatively and nonoperatively and to provide an updated rehabilitation treatment algorithm.
Methods: Studies were identified by searching the MEDLINE database from 01/1995 to 09/2020. Included studies contained detailed rehabilitation protocols with physiologic rationale for AC joint injuries. Biomechanical studies, technique articles, radiographic studies, systematic reviews, case studies, editorials, and studies that compared nonoperative versus operative treatment without focus on rehabilitation were excluded. Following identification of the literature, an updated treatment algorithm was created.
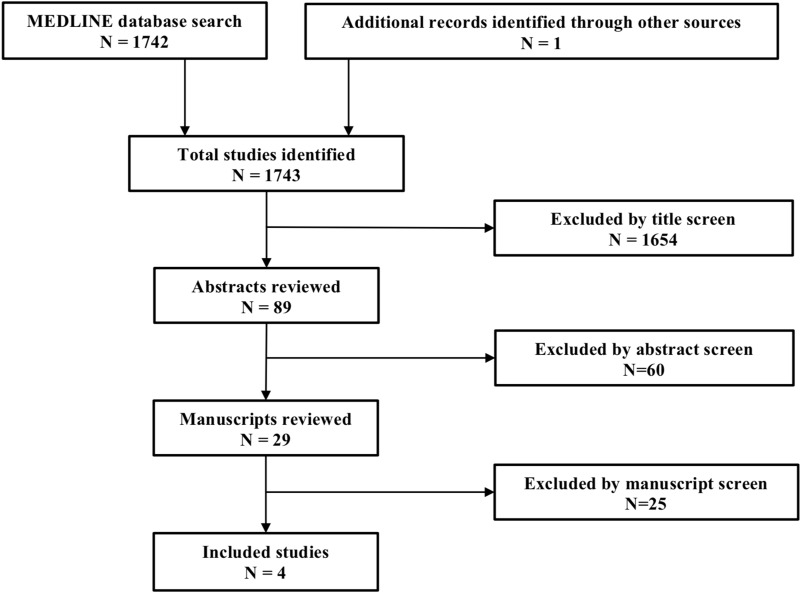
Results: The search strategy yielded 1742 studies, of which 1654 studies were excluded based on title, 60 on the abstract, and 25 on the full manuscript. One study was manually identified using article reference lists, yielding four publications presenting detailed rehabilitation protocols based on physiologic rationale. No randomized controlled trials or comparative studies were identified or cited as a basis for these rehabilitation protocols.
Conclusion: Few detailed rehabilitation protocols in patients with AC joint injuries have been published. These protocols are limited by their standardization, arbitrary timelines, and provide minimal assessment of individual patient characteristics. The quality of patient care can be improved with more practical guidelines that are goal-oriented and allow for critical thinking among clinicians to address individual patient needs. Three common barriers preventing successful rehabilitation were identified and addressed: Pain, Apprehension, and (anterior chest wall) Stiffness to regain Scapular control, effectively termed "PASS" for AC joint rehabilitation.
Clinical relevance: Rehabilitation protocols for AC joint injuries should be less formulaic and instead allow for critical thinking and effective communication among clinicians and therapists to address individual patient needs.
Keywords: AC joint; acromioclavicular joint; physical therapy; rehabilitation.
© 2021 LeVasseur et al.
Conflict of interest statement
LeVasseur MR, Mancini MR, Berthold DP, Cusano A, McCann GP, and Gomlinski G declare that they have no conflict of interest. Cote MP receives personal fees from Arthroscopy Association of North America (AANA) outside of the submitted work. Mazzocca AD reports research grants from Arthrex Inc. outside the submitted work and is a consultant for Arthrex Inc. The authors report no other potential conflicts of interest for this work. This investigation was performed at the Department of Orthopaedic Surgery, University of Connecticut, Farmington, Connecticut, USA.
Figures


Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Horizontal Instability of the Acromioclavicular Joint: A Systematic Review.Am J Sports Med. 2020 Feb;48(2):504-510. doi: 10.1177/0363546519831013. Epub 2019 Apr 23. Am J Sports Med. 2020. PMID: 31013137
-
Criteria for return to play after operative management of acromioclavicular joint separation: a systematic review.JSES Rev Rep Tech. 2021 Dec 31;2(2):140-148. doi: 10.1016/j.xrrt.2021.11.005. eCollection 2022 May. JSES Rev Rep Tech. 2021. PMID: 37587962 Free PMC article. Review.
-
Acromioclavicular Joint Injuries: Evidence-based Treatment.J Am Acad Orthop Surg. 2019 Sep 1;27(17):e775-e788. doi: 10.5435/JAAOS-D-17-00105. J Am Acad Orthop Surg. 2019. PMID: 31008872 Review.
-
Decision making: operative versus nonoperative treatment of acromioclavicular joint injuries.Clin Sports Med. 2003 Apr;22(2):277-90. doi: 10.1016/s0278-5919(02)00098-4. Clin Sports Med. 2003. PMID: 12825530 Review.
Cited by
-
Management of Common Football-Related Injuries About the Shoulder.HSS J. 2023 Aug;19(3):339-350. doi: 10.1177/15563316231172107. Epub 2023 May 20. HSS J. 2023. PMID: 37435133 Free PMC article. No abstract available.
-
Distal Clavicle Osteolysis in a 30-Year-Old Male: A Case Report.Cureus. 2025 May 23;17(5):e84697. doi: 10.7759/cureus.84697. eCollection 2025 May. Cureus. 2025. PMID: 40551918 Free PMC article.
-
Management of Acromioclavicular Injuries - Current Concepts.Orthop Res Rev. 2023 Feb 16;15:1-12. doi: 10.2147/ORR.S340531. eCollection 2023. Orthop Res Rev. 2023. PMID: 36814992 Free PMC article. Review.
-
Multimodal Exercises Adjunct to Virtual Reality in Acromioclavicular Joint Sprain Rehabilitation: A Case Report.Cureus. 2024 Aug 10;16(8):e66599. doi: 10.7759/cureus.66599. eCollection 2024 Aug. Cureus. 2024. PMID: 39258074 Free PMC article.
-
Effectiveness of proprioceptive neuromuscular facilitation pattern on upper extremity and scapula in patients with adhesive capsulitis: a single-centre assessor-blinded randomised controlled trial (RCT).Trials. 2025 May 3;26(1):146. doi: 10.1186/s13063-025-08848-0. Trials. 2025. PMID: 40317031 Free PMC article. Clinical Trial.
References
-
- Rockwood CA, Williams GR, Young DC. Disorders of the acromioclavicular joint. In: Rockwood CA, Matsen FA, editors. The Shoulder. Philadelphia: Saunders; 1998:483–553.
Publication types
LinkOut - more resources
Full Text Sources
