

Clinical Utility of Transcranial Magnetic Stimulation (TMS) in the Presurgical Evaluation of Motor, Speech, and Language Functions in Young Children With Refractory Epilepsy or Brain Tumor: Preliminary Evidence
- PMID: 34093397
- PMCID: PMC8170483
- DOI: 10.3389/fneur.2021.650830
Clinical Utility of Transcranial Magnetic Stimulation (TMS) in the Presurgical Evaluation of Motor, Speech, and Language Functions in Young Children With Refractory Epilepsy or Brain Tumor: Preliminary Evidence
Abstract
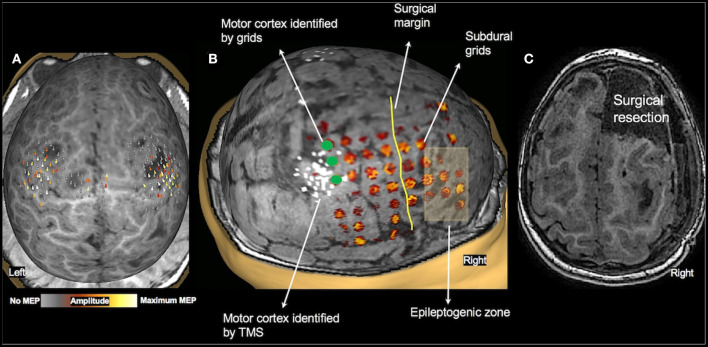
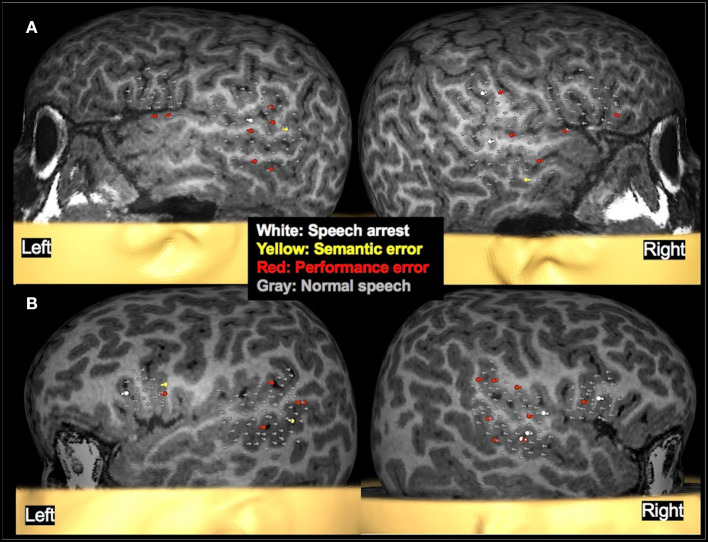
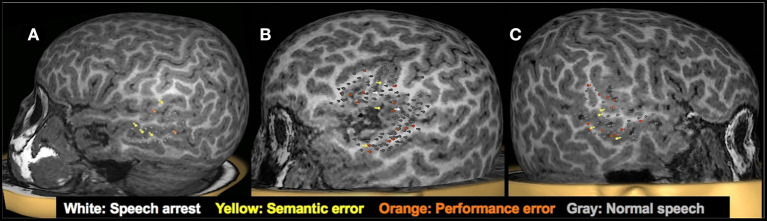
Accurate presurgical mapping of motor, speech, and language cortices, while crucial for neurosurgical planning and minimizing post-operative functional deficits, is challenging in young children with neurological disease. In such children, both invasive (cortical stimulation mapping) and non-invasive functional mapping imaging methods (MEG, fMRI) have limited success, often leading to delayed surgery or adverse post-surgical outcomes. We therefore examined the clinical utility of transcranial magnetic stimulation (TMS) in young children who require functional mapping. In a retrospective chart review of TMS studies performed on children with refractory epilepsy or a brain tumor, at our institution, we identified 47 mapping sessions in 36 children 3 years of age or younger, in whom upper and lower extremity motor mapping was attempted; and 13 children 5-6 years old in whom language mapping, using a naming paradigm, was attempted. The primary hand motor cortex was identified in at least one hemisphere in 33 of 36 patients, and in both hemispheres in 27 children. In 17 children, primary leg motor cortex was also successfully identified. The language cortices in temporal regions were successfully mapped in 11 of 13 patients, and in six of them language cortices in frontal regions were also mapped, with most children (n = 5) showing right hemisphere dominance for expressive language. Ten children had a seizure that was consistent with their clinical semiology during or immediately following TMS, none of which required intervention or impeded completion of mapping. Using TMS, both normal motor, speech, and language developmental patterns and apparent disease induced reorganization were demonstrated in this young cohort. The successful localization of motor, speech, and language cortices in young children improved the understanding of the risk-benefit ratio prior to surgery and facilitated surgical planning aimed at preserving motor, speech, and language functions. Post-operatively, motor function was preserved or improved in nine out of 11 children who underwent surgery, as was language function in all seven children who had surgery for lesions near eloquent cortices. We provide feasibility data that TMS is a safe, reliable, and effective tool to map eloquent cortices in young children.
Keywords: brain tumor; children; epilepsy; language mapping; motor mapping; presurgical; speech mapping; transcranial magnetic stimulation.
Copyright © 2021 Narayana, Gibbs, Fulton, McGregor, Mudigoudar, Weatherspoon, Boop and Wheless.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Noninvasive Localization of Language Cortex in an Awake 4-Year-Old Child with Rasmussen Encephalitis: A Case Report.Oper Neurosurg. 2020 May 1;18(5):E175-E180. doi: 10.1093/ons/opz202. Oper Neurosurg. 2020. PMID: 31342072
-
The Clinical Utility of Transcranial Magnetic Stimulation in Determining Hemispheric Dominance for Language: A Magnetoencephalography Comparison Study.J Clin Neurophysiol. 2020 Mar;37(2):90-103. doi: 10.1097/WNP.0000000000000499. J Clin Neurophysiol. 2020. PMID: 32142020
-
Concordance Between Transcranial Magnetic Stimulation and Functional Magnetic Resonance Imaging (MRI) Derived Localization of Language in a Clinical Cohort.J Child Neurol. 2020 May;35(6):363-379. doi: 10.1177/0883073820901415. Epub 2020 Mar 3. J Child Neurol. 2020. PMID: 32122221
-
[Navigated transcranial magnetic stimulation for preoperative mapping of the eloquent cortex].Nervenarzt. 2015 Dec;86(12):1508-15. doi: 10.1007/s00115-015-4316-7. Nervenarzt. 2015. PMID: 26452779 Review. German.
-
Current status and potential application of navigated transcranial magnetic stimulation in neurosurgery: a literature review.Chin Neurosurg J. 2019 May 21;5:12. doi: 10.1186/s41016-019-0159-6. eCollection 2019. Chin Neurosurg J. 2019. PMID: 32922912 Free PMC article. Review.
Cited by
-
Cellular Mechanisms of Electromagnetic Field in Traumatic Brain Injury.J Biotechnol Biomed. 2023;6(2):95-104. doi: 10.26502/jbb.2642-91280075. Epub 2023 Apr 7. J Biotechnol Biomed. 2023. PMID: 37388676 Free PMC article.
-
The functional near infrared spectroscopy applications in children with developmental diseases: a review.Front Neurol. 2025 Jun 17;16:1495138. doi: 10.3389/fneur.2025.1495138. eCollection 2025. Front Neurol. 2025. PMID: 40599736 Free PMC article. Review.
-
Surgery for pediatric drug resistant epilepsy: a narrative review of its history, surgical implications, and treatment strategies.Transl Pediatr. 2023 Feb 28;12(2):245-259. doi: 10.21037/tp-22-200. Epub 2023 Feb 13. Transl Pediatr. 2023. PMID: 36891373 Free PMC article. Review.
-
Single-pulse transcranial magnetic stimulation for assessment of motor development in infants with early brain injury.Expert Rev Med Devices. 2024 Mar;21(3):179-186. doi: 10.1080/17434440.2023.2299310. Epub 2024 Jan 3. Expert Rev Med Devices. 2024. PMID: 38166497 Free PMC article.
-
Transcranial Magnetic Stimulation-Electroencephalography (TMS-EEG) in Neurosurgery: Unexplored Path Towards Personalized Brain Surgery.J Pers Med. 2024 Dec 9;14(12):1144. doi: 10.3390/jpm14121144. J Pers Med. 2024. PMID: 39728057 Free PMC article. Review.
References
-
- Szaflarski JP, Gloss D, Binder JR, Gaillard WD, Golby AJ, Holland SK, et al. . Practice guideline summary: use of fMRI in the presurgical evaluation of patients with epilepsy: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology. (2017) 88:395–402. 10.1212/WNL.0000000000003532 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Medical