

Improvement in Midline Shift Is a Positive Prognostic Predictor for Malignant Middle Cerebral Artery Infarction Patients Undergoing Decompressive Craniectomy
- PMID: 34093400
- PMCID: PMC8176305
- DOI: 10.3389/fneur.2021.652827
Improvement in Midline Shift Is a Positive Prognostic Predictor for Malignant Middle Cerebral Artery Infarction Patients Undergoing Decompressive Craniectomy
Abstract
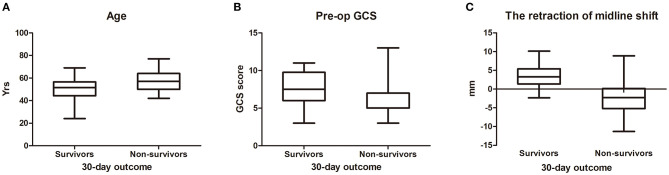
Objective: The aim of this retrospective study is to evaluate the risk factors of malignant middle cerebral artery infarction (MMCAI) patients and explore an applicable prognostic predictor for MMCAI patients undergoing decompressive craniectomy (DC). Methods: Clinical data from the period 2012-2017 were retrospectively evaluated. Forty-three consecutive MMCAI patients undergoing DC were enrolled in this study. The 30-day mortality was assessed, and age, location, hypertension, pupil dilation, onset to operation duration, midline shift, and Glasgow Coma Scale (GCS) score were identified by univariate analysis and binary logistic regression. Results: In this retrospective study for DC patients, the 30-day mortality was 44.2%. In the univariate analysis, advanced age (≥60 years), right hemispheric location, hypertension, pupil dilation, shorter onset to operation duration (<48 h), improved midline shift (t = 4.214, p < 0.01), and lower pre-operation GCS score were significant predictors of death within 30 days. In binary logistic regression analysis, age [odds ratio (OR) = 1.141, 95% CI 1.011-1.287], the improvement of the midline shift (OR = 0.764, 95% CI 0.59-0.988), and pupillary dilation (OR = 15.10, 95% CI 1.374-165.954) were independent influencing factors. For the receiver operating characteristic (ROC) analysis of the relationship between post-operation outcomes and midline shift improvement, the area under the curve (AUC) was 0.844, and the cutoff point of midline shift improvement was 0.83 cm. Conclusion: Improved midline shift was a significant predictor of 30-day mortality. The improved midline shift of >0.83 cm indicated survival at 30 days.
Keywords: decompressive craniectomy; hypertensive intracerebral hemorrhage; improvement in midline shift; malignant middle cerebral artery infarction; mortality.
Copyright © 2021 Chen, Hao, Yang, Wang, Zhao, Zhang, Ye and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Timing of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Single-Center Analysis.Medicina (Kaunas). 2019 Jan 30;55(2):31. doi: 10.3390/medicina55020031. Medicina (Kaunas). 2019. PMID: 30704138 Free PMC article.
-
Association Between Preoperative Midline Shift Growing Rate and Outcomes of Decompressive Craniectomy in Patients with Malignant Middle Cerebral Artery Infarction.Curr Neurovasc Res. 2020;17(2):131-139. doi: 10.2174/1567202617666200207125552. Curr Neurovasc Res. 2020. PMID: 32031070
-
Decompressive hemicraniectomy for malignant middle cerebral artery infarction including patients with additional involvement of the anterior and/or posterior cerebral artery territory-outcome analysis and definition of prognostic factors.Acta Neurochir (Wien). 2018 Jan;160(1):83-89. doi: 10.1007/s00701-017-3329-3. Epub 2017 Sep 30. Acta Neurochir (Wien). 2018. PMID: 28965156
-
Outcome After Decompressive Craniectomy for Middle Cerebral Artery Infarction: Timing of the Intervention.Neurosurgery. 2020 Mar 1;86(3):E318-E325. doi: 10.1093/neuros/nyz522. Neurosurgery. 2020. PMID: 31943069 Free PMC article.
-
Assessment of outcome following decompressive craniectomy for malignant middle cerebral artery infarction in patients older than 60 years of age.Neurosurg Focus. 2009 Jun;26(6):E3. doi: 10.3171/2009.3.FOCUS0958. Neurosurg Focus. 2009. PMID: 19485716 Review.
References
LinkOut - more resources
Full Text Sources