

Tumor Necrosis Factor Inhibitors Exacerbate Whipple's Disease by Reprogramming Macrophage and Inducing Apoptosis
- PMID: 34093562
- PMCID: PMC8173622
- DOI: 10.3389/fimmu.2021.667357
Tumor Necrosis Factor Inhibitors Exacerbate Whipple's Disease by Reprogramming Macrophage and Inducing Apoptosis
Abstract
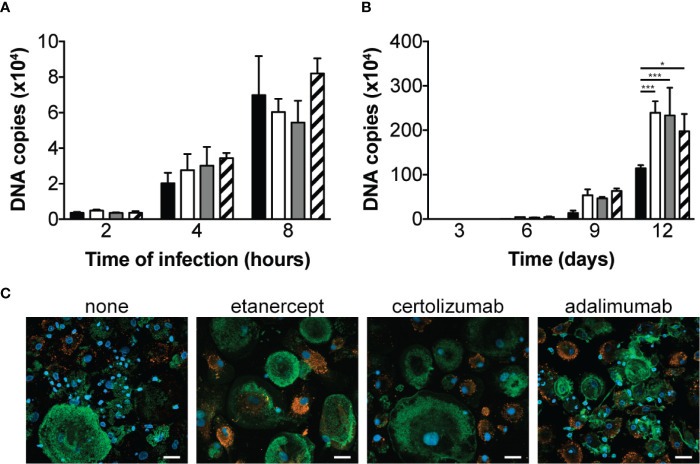
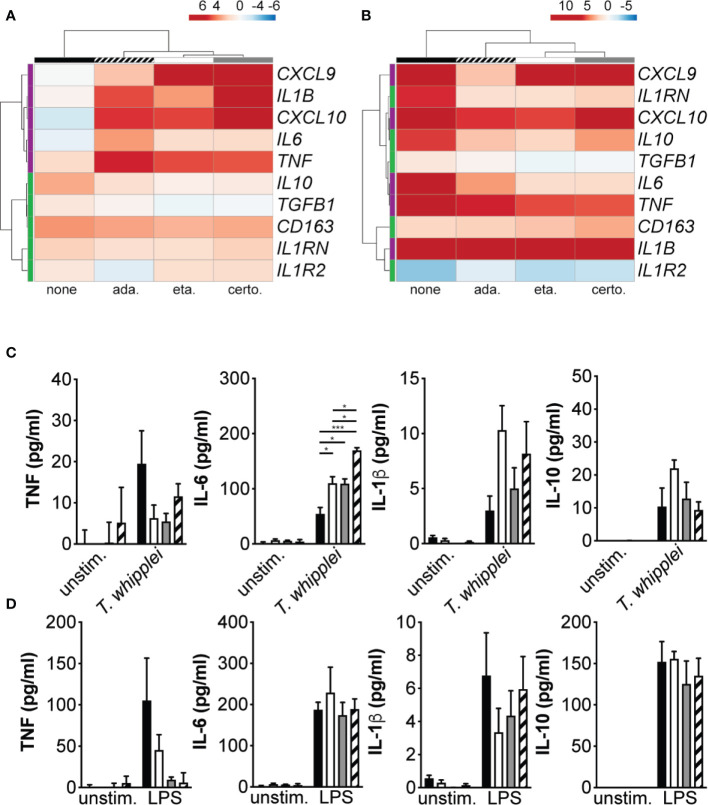
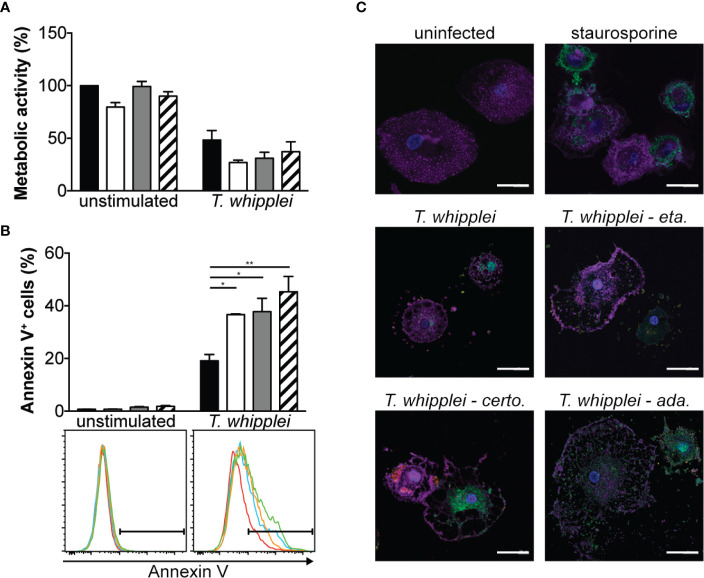
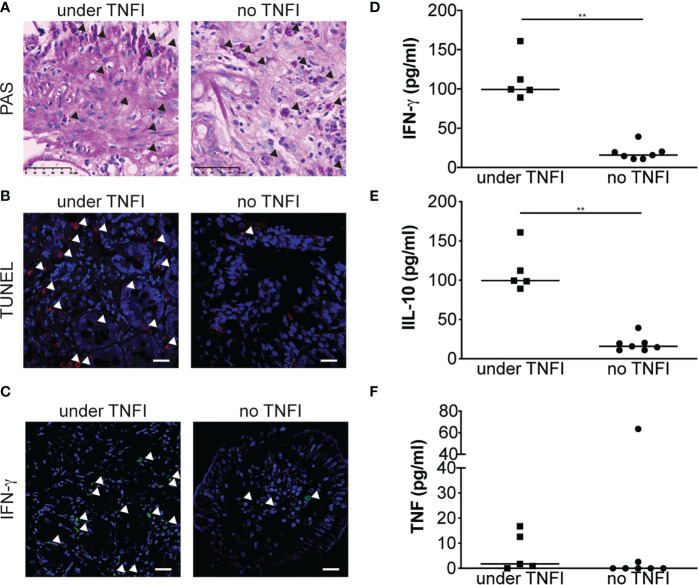
Tropheryma whipplei is the agent of Whipple's disease, a rare systemic disease characterized by macrophage infiltration of the intestinal mucosa. The disease first manifests as arthralgia and/or arthropathy that usually precede the diagnosis by years, and which may push clinicians to prescribe Tumor necrosis factor inhibitors (TNFI) to treat unexplained arthralgia. However, such therapies have been associated with exacerbation of subclinical undiagnosed Whipple's disease. The objective of this study was to delineate the biological basis of disease exacerbation. We found that etanercept, adalimumab or certolizumab treatment of monocyte-derived macrophages from healthy subjects significantly increased bacterial replication in vitro without affecting uptake. Interestingly, this effect was associated with macrophage repolarization and increased rate of apoptosis. Further analysis revealed that in patients for whom Whipple's disease diagnosis was made while under TNFI therapy, apoptosis was increased in duodenal tissue specimens as compared with control Whipple's disease patients who never received TNFI prior diagnosis. In addition, IFN-γ expression was increased in duodenal biopsy specimen and circulating levels of IFN-γ were higher in patients for whom Whipple's disease diagnosis was made while under TNFI therapy. Taken together, our findings establish that TNFI aggravate/exacerbate latent or subclinical undiagnosed Whipple's disease by promoting a strong inflammatory response and apoptosis and confirm that patients may be screened for T. whipplei prior to introduction of TNFI therapy.
Keywords: IFNγ; TNF inhibitor; Tropheryma whipplei; Whipple’s disease; macrophages.
Copyright © 2021 Boumaza, Mezouar, Bardou, Raoult, Mège and Desnues.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Impaired immune functions of monocytes and macrophages in Whipple's disease.Gastroenterology. 2010 Jan;138(1):210-20. doi: 10.1053/j.gastro.2009.07.066. Epub 2009 Aug 5. Gastroenterology. 2010. PMID: 19664628
-
Specific and nonspecific B-cell function in the small intestines of patients with Whipple's disease.Infect Immun. 2010 Nov;78(11):4589-92. doi: 10.1128/IAI.00705-10. Epub 2010 Aug 9. Infect Immun. 2010. PMID: 20696822 Free PMC article.
-
[Diagnostic issues of Whipple's disease during chronic inflammatory rheumatism: About three cases].Rev Med Interne. 2021 Nov;42(11):801-804. doi: 10.1016/j.revmed.2021.06.009. Epub 2021 Jul 1. Rev Med Interne. 2021. PMID: 34218934 French.
-
Changing paradigms in Whipple's disease and infection with Tropheryma whipplei.Eur J Clin Microbiol Infect Dis. 2011 Oct;30(10):1151-8. doi: 10.1007/s10096-011-1209-y. Epub 2011 Apr 2. Eur J Clin Microbiol Infect Dis. 2011. PMID: 21461659 Review.
-
Whipple's arthritis.Joint Bone Spine. 2016 Dec;83(6):631-635. doi: 10.1016/j.jbspin.2016.07.001. Epub 2016 Aug 5. Joint Bone Spine. 2016. PMID: 27502365 Review.
Cited by
-
Use of bevacizumab in a patient with Whipple's disease: managing diagnostic uncertainty.BMJ Case Rep. 2023 Oct 24;16(10):e256460. doi: 10.1136/bcr-2023-256460. BMJ Case Rep. 2023. PMID: 37879715
-
Current knowledge of the immune reconstitution inflammatory syndrome in Whipple disease: a review.Front Immunol. 2023 Oct 13;14:1265414. doi: 10.3389/fimmu.2023.1265414. eCollection 2023. Front Immunol. 2023. PMID: 37901208 Free PMC article. Review.
-
The crucial regulatory role of type I interferon in inflammatory diseases.Cell Biosci. 2023 Dec 20;13(1):230. doi: 10.1186/s13578-023-01188-z. Cell Biosci. 2023. PMID: 38124132 Free PMC article. Review.
-
Diagnosis of Whipple's disease with pseudorheumatoid nodules in a patient treated with biologics for rheumatoid polyarthritis.Rheumatol Adv Pract. 2023 Jan 10;7(1):rkad002. doi: 10.1093/rap/rkad002. eCollection 2023. Rheumatol Adv Pract. 2023. PMID: 36726734 Free PMC article. No abstract available.
-
Whipple's disease unmasked by TNF inhibitor therapy for treatment of seronegative rheumatoid arthritis.BMJ Case Rep. 2022 Jul 21;15(7):e250693. doi: 10.1136/bcr-2022-250693. BMJ Case Rep. 2022. PMID: 35863856 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources