

Use of pressure-regulated volume control in the first 48 hours of hospitalization of mechanically ventilated patients with sepsis or septic shock, with or without ARDS
- PMID: 34093732
- PMCID: PMC8142092
- DOI: 10.1177/1751143719878969
Use of pressure-regulated volume control in the first 48 hours of hospitalization of mechanically ventilated patients with sepsis or septic shock, with or without ARDS
Abstract
Purpose: To evaluate the impact of pressure-regulated volume control (PRVC/VC+) use on delivered tidal volumes in patients with acute respiratory distress syndrome (ARDS) or at risk for ARDS.
Materials and methods: Retrospective study of mechanically ventilated adult patients with severe sepsis or septic shock.
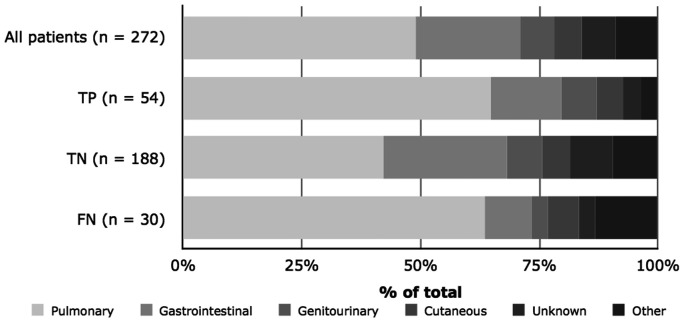
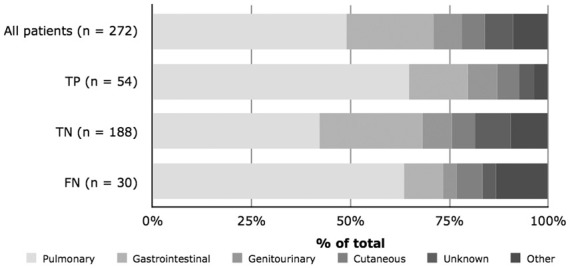
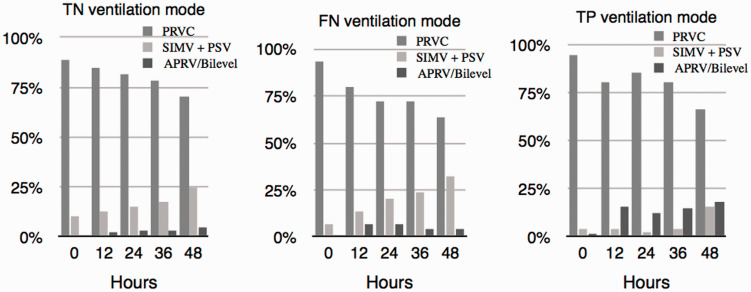
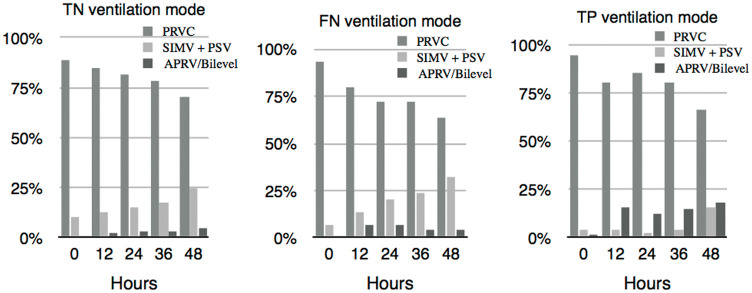
Results: A total of 272 patients were divided into patients with recognized ARDS, patients without ARDS, and patients with unrecognized ARDS. Over 90% of patients were ventilated with PRVC on admission, resulting in delivered tidal volumes significantly higher than set tidal volumes among all groups at all time points, even after ARDS recognition (p < 0.001). Tidal volumes were lower for patients with pulmonary sepsis as compared to those with a nonpulmonary origin (p < 0.001).
Conclusions: Using PRVC promotes augmented delivered tidal volumes, often in excess of 6 mL/kg ideal body weight. Correct recognition of ARDS and having pulmonary sepsis improves compliance with low-stretch protocol ventilation.
Keywords: Acute respiratory distress syndrome; adult; artificial; critical care; respiration; sepsis; septic; shock; ventilator-induced lung injury.
© The Intensive Care Society 2019.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af. Crit Care Med. 2013. PMID: 23353941
-
The impact of cardiac dysfunction on acute respiratory distress syndrome and mortality in mechanically ventilated patients with severe sepsis and septic shock: an observational study.J Crit Care. 2015 Feb;30(1):65-70. doi: 10.1016/j.jcrc.2014.07.027. Epub 2014 Aug 7. J Crit Care. 2015. PMID: 25179413 Free PMC article.
-
Sepsis-associated pulmonary complications in emergency department patients monitored with serial lactate: An observational cohort study.J Crit Care. 2015 Dec;30(6):1163-8. doi: 10.1016/j.jcrc.2015.07.031. Epub 2015 Aug 1. J Crit Care. 2015. PMID: 26362864 Free PMC article.
-
Driving Pressure-limited Strategy for Patients with Acute Respiratory Distress Syndrome. A Pilot Randomized Clinical Trial.Ann Am Thorac Soc. 2020 May;17(5):596-604. doi: 10.1513/AnnalsATS.201907-506OC. Ann Am Thorac Soc. 2020. PMID: 32069068 Clinical Trial.
-
Lung-protective mechanical ventilation with lower tidal volumes in patients not suffering from acute lung injury: a review of clinical studies.Med Sci Monit. 2008 Feb;14(2):RA22-26. Med Sci Monit. 2008. PMID: 18227773 Review.
Cited by
-
Smoking on the risk of acute respiratory distress syndrome: a systematic review and meta-analysis.Crit Care. 2024 Apr 14;28(1):122. doi: 10.1186/s13054-024-04902-6. Crit Care. 2024. PMID: 38616271 Free PMC article.
-
Comparison of Ventilation Strategies Across the Perioperative Period in Patients Undergoing General Anesthesia: A Narrative Review.Cureus. 2025 Jan 20;17(1):e77728. doi: 10.7759/cureus.77728. eCollection 2025 Jan. Cureus. 2025. PMID: 39974262 Free PMC article. Review.
-
Adaptive Pressure Control-Continuous Mandatory Ventilation Versus Volume Control-Continuous Mandatory Ventilation: Factors Associated With Initiation, Maintenance, and Adjustment.Respir Care. 2024 Nov 18;69(12):1491-1498. doi: 10.4187/respcare.11430. Respir Care. 2024. PMID: 39107061
References
-
- The ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin definition. JAMA 2012; 307: 2526–2533. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med 2005; 353: 1685–1693. - PubMed
-
- Stewart TE, Meade MO, Cook DJ, et al. Evaluation of a ventilation strategy to prevent barotrauma in patients at high risk for Acute Respiratory Distress Syndrome. N Engl J Med 1998; 338: 355–361. - PubMed
-
- Gajic O, Dara SI, Mendez JL, et al. Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation. Crit Care Med 2004; 32: 1817–1824. - PubMed
-
- Girard TD, Bernard GR. Mechanical ventilation in ARDS – a state-of-the-art review. Chest 2007; 131: 921–929. - PubMed
LinkOut - more resources
Full Text Sources