

INSL4 as prognostic marker for proliferation and invasiveness in Non-Small-Cell Lung Cancer
- PMID: 34093787
- PMCID: PMC8176261
- DOI: 10.7150/jca.51332
INSL4 as prognostic marker for proliferation and invasiveness in Non-Small-Cell Lung Cancer
Abstract
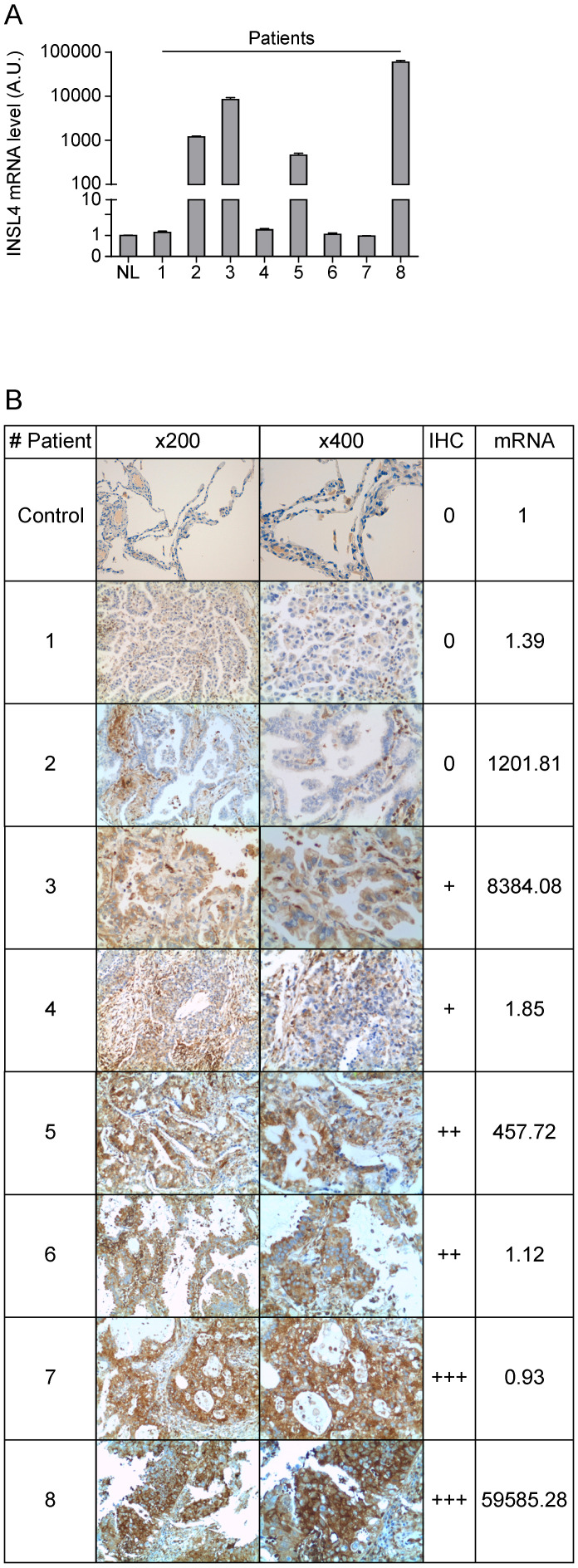
Non-small-cell-lung cancer accounts for 80-85% of all forms of lung cancer as leading cause of cancer-related death in human. Despite remarkable advances in the diagnosis and therapy of lung cancer, no significant improvements have thus far been achieved in terms of patients' prognosis. Here, we investigated the role of INSL4 - a member of the relaxin-family - in NSCLC. We overexpressed INSL4 in NSCLC cells to analyse in vitro the growth rate and the tumourigenic features. We investigated the signalling pathways engaged in INSL4 overexpressing cells and the tumour growth ability by studying the tumour development in a patient derived tumour xenograft mouse model. We found an INSL4 cell growth promoting effect in vitro in H1299 cells and in vivo in NOD/SCID mice. Surprisingly, in NSCLC-A549 cells, INSL4 overexpression has not similar effect, despite huge basal INSL4-mRNA expression respect to H1299. The INSL4-mRNA analysis of eight different NSCLC-derived cell lines, revealed highly difference in the INSL4-mRNA amount. Transfection of NSCLC lines with INSL4-Myc showed huge level of INSL4-mRNA with a very low amount of protein expressed. Notably, similar discrepancy has been observed in NSCLC patients. However, in a cohort of NSCLC patients analysing a database, we found a significant inverse correlation between INSL4 expression and Overall Survival. By combining the in vitro and in vivo results, suggest that in patients whose NSCLC adenocarcinoma spontaneously expressed high levels of INSL4 post-transcriptional modifications affecting INSL4 do not allow to assess precision therapy in selected patients without consider protein INSL4 amount.
Keywords: INSL4; NSCLC adenocarcinoma; invasiveness; proliferation; xenograft mouse.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures





Similar articles
-
Role of INSL4 Signaling in Sustaining the Growth and Viability of LKB1-Inactivated Lung Cancer.J Natl Cancer Inst. 2019 Jul 1;111(7):664-674. doi: 10.1093/jnci/djy166. J Natl Cancer Inst. 2019. PMID: 30423141 Free PMC article.
-
Protein tyrosine phosphatase PTPRB regulates Src phosphorylation and tumour progression in NSCLC.Clin Exp Pharmacol Physiol. 2016 Oct;43(10):1004-12. doi: 10.1111/1440-1681.12610. Clin Exp Pharmacol Physiol. 2016. PMID: 27314562
-
Interleukin-37 suppresses tumor growth through inhibition of angiogenesis in non-small cell lung cancer.J Exp Clin Cancer Res. 2016 Jan 20;35:13. doi: 10.1186/s13046-016-0293-3. J Exp Clin Cancer Res. 2016. PMID: 26791086 Free PMC article.
-
Modification of α2,6-sialylation mediates the invasiveness and tumorigenicity of non-small cell lung cancer cells in vitro and in vivo via Notch1/Hes1/MMPs pathway.Int J Cancer. 2018 Nov 1;143(9):2319-2330. doi: 10.1002/ijc.31737. Epub 2018 Sep 7. Int J Cancer. 2018. PMID: 29981167
-
Insulin-like 4 (INSL4) gene expression in human embryonic and trophoblastic tissues.Mol Reprod Dev. 1998 Oct;51(2):123-9. doi: 10.1002/(SICI)1098-2795(199810)51:2<123::AID-MRD1>3.0.CO;2-S. Mol Reprod Dev. 1998. PMID: 9740319
Cited by
-
Identification of cuproptosis-related gene signature to predict prognosis in lung adenocarcinoma.Front Genet. 2022 Oct 14;13:1016871. doi: 10.3389/fgene.2022.1016871. eCollection 2022. Front Genet. 2022. PMID: 36313444 Free PMC article.
-
AGTR1: a potential biomarker associated with the occurrence and prognosis of lung adenocarcinoma.Front Oncol. 2024 Oct 10;14:1441235. doi: 10.3389/fonc.2024.1441235. eCollection 2024. Front Oncol. 2024. PMID: 39450258 Free PMC article.
-
Development and validation of an immune-related gene signature for prognosis in Lung adenocarcinoma.IET Syst Biol. 2023 Feb;17(1):27-38. doi: 10.1049/syb2.12057. Epub 2023 Feb 2. IET Syst Biol. 2023. PMID: 36728032 Free PMC article.
-
Mutations, inflammation and phenotype of myeloproliferative neoplasms.Front Oncol. 2023 May 22;13:1196817. doi: 10.3389/fonc.2023.1196817. eCollection 2023. Front Oncol. 2023. PMID: 37284191 Free PMC article. Review.
-
Construction of a lung adenocarcinoma prognostic model based on KEAP1/NRF2/HO‑1 mutation‑mediated upregulated genes and bioinformatic analysis.Oncol Lett. 2025 Jan 23;29(3):155. doi: 10.3892/ol.2025.14902. eCollection 2025 Mar. Oncol Lett. 2025. PMID: 39911153 Free PMC article.
References
-
- Navada S, Lai P, Schwartz AG, Kalemkerian GP. Temporal trends in small cell lung cancer: Analysis of the national Surveillance, Epidemiology, and End-Results (SEER) database. J Clin Oncol. 2006;24:384s–s.
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA: a cancer journal for clinicians. 2012;62:10–29. - PubMed
-
- Torre LA, Bray F, Siegel RL. et al. Global cancer statistics, 2012. CA: a cancer journal for clinicians. 2015;65:87–108. - PubMed
LinkOut - more resources
Full Text Sources
