

A novel risk-scoring system conducing to chemotherapy decision for patients with pancreatic ductal adenocarcinoma after pancreatectomy
- PMID: 34093844
- PMCID: PMC8176415
- DOI: 10.7150/jca.57768
A novel risk-scoring system conducing to chemotherapy decision for patients with pancreatic ductal adenocarcinoma after pancreatectomy
Abstract
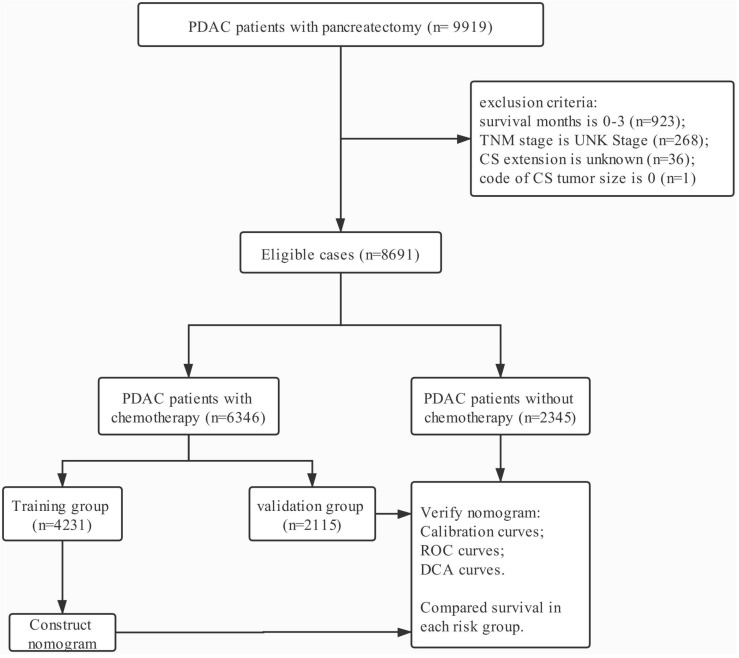
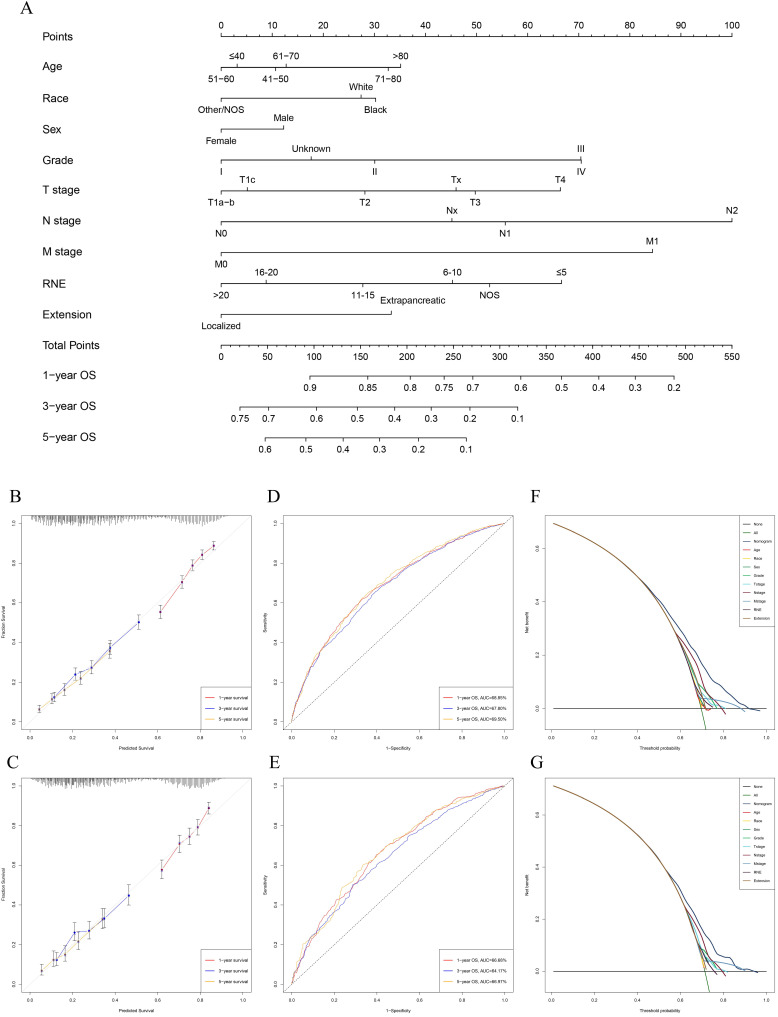
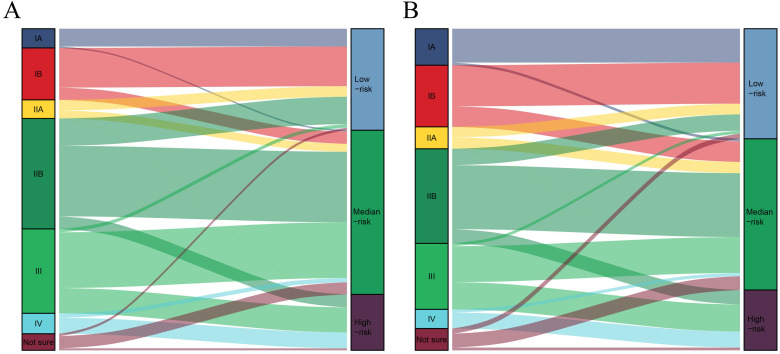
Background: Chemotherapy is suggested to use in all stages of pancreatic cancer. Is it reasonable to recommend chemotherapy for all PDAC patients? It is necessary to distinguish low-risk PDAC patients underwent pancreatectomy, who may not lose survival time due to missed chemotherapy and not need to endure pain, nausea, tiredness, drowsiness, and breath shortness caused by chemotherapy. Methods: Nomograms were constructed with basis from the multivariate Cox regression analysis. X-tile software was utilized to perform risk stratification. Survival curves were used to display the effect of chemotherapy in different risk-stratification. Results: All of the significant variables were used to create the nomograms for overall survival (OS). The total risk score of each patient was calculated by summing the scores related to each variable. X-tile software was utilized to classify patients into high-risk (score >283), median-risk (197<score ≤283), and low-risk (score ≤197) according to the total risk score. The low-risk PDAC patients after pancreatectomy cannot gain survival benefit from chemotherapy after surgery (p=0.443). Moreover, chemotherapy improved survival for patients with resected PDAC in the median-risk (p<0.001) and high-risk (p<0.001) groups. Conclusions: our research constructed a new risk-scoring system based on survival nomogram to screen low-risk PDAC patients after pancreatectomy and confirmed that those can avoid enduring side effects caused by chemotherapy without affecting the survival time.
Keywords: PDAC; SEER database; chemotherapy; nomogram; surgical resection.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures

Similar articles
-
Effects of Total Pancreatectomy on Survival of Patients With Pancreatic Ductal Adenocarcinoma: A Population-Based Study.Front Surg. 2021 Dec 9;8:804785. doi: 10.3389/fsurg.2021.804785. eCollection 2021. Front Surg. 2021. PMID: 34957210 Free PMC article.
-
Development and validation of novel nomograms for predicting the survival of patients after surgical resection of pancreatic ductal adenocarcinoma.Cancer Med. 2020 May;9(10):3353-3370. doi: 10.1002/cam4.2959. Epub 2020 Mar 17. Cancer Med. 2020. PMID: 32181599 Free PMC article.
-
Effect of neoadjuvant radiotherapy on survival of non-metastatic pancreatic ductal adenocarcinoma: a SEER database analysis.Radiat Oncol. 2020 May 13;15(1):107. doi: 10.1186/s13014-020-01561-z. Radiat Oncol. 2020. PMID: 32404114 Free PMC article.
-
Pancreatic ductal adenocarcinoma: a radiomics nomogram outperforms clinical model and TNM staging for survival estimation after curative resection.Eur Radiol. 2020 May;30(5):2513-2524. doi: 10.1007/s00330-019-06600-2. Epub 2020 Jan 31. Eur Radiol. 2020. PMID: 32006171
-
Repeated Pancreatectomy for Isolated Local Recurrence in the Remnant Pancreas Following Radical Pancreatectomy for Pancreatic Ductal Adenocarcinoma: A Pooled Analysis.J Clin Med. 2020 Dec 5;9(12):3945. doi: 10.3390/jcm9123945. J Clin Med. 2020. PMID: 33291378 Free PMC article. Review.
Cited by
-
Development and external validation of a prognostic nomogram to predict survival in patients aged ≥60 years with pancreatic ductal adenocarcinoma.Transl Cancer Res. 2024 Jun 30;13(6):2751-2766. doi: 10.21037/tcr-24-5. Epub 2024 Jun 13. Transl Cancer Res. 2024. PMID: 38988930 Free PMC article.
-
Establishment and validation of nomogram models for overall survival and cancer-specific survival in spindle cell sarcoma patients.Sci Rep. 2023 Dec 27;13(1):23018. doi: 10.1038/s41598-023-50401-z. Sci Rep. 2023. PMID: 38155261 Free PMC article.
References
-
- Bailey P, Chang DK, Nones K, Johns AL, Patch AM, Gingras MC. et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature. 2016;531:47–52. - PubMed
-
- Hidalgo M, Cascinu S, Kleeff J, Labianca R, Lohr JM, Neoptolemos J. et al. Addressing the challenges of pancreatic cancer: future directions for improving outcomes. Pancreatology: official journal of the International Association of Pancreatology. 2015;15:8–18. - PubMed
-
- Tempero MA, Malafa MP, Chiorean EG, Czito B, Scaife C, Narang AK. et al. Pancreatic Adenocarcinoma, Version 1.2019. Journal of the National Comprehensive Cancer Network: JNCCN. 2019;17:202–10. - PubMed
LinkOut - more resources
Full Text Sources
