

Preoperative Gadoxetic Acid-Enhanced MRI Based Nomogram Improves Prediction of Early HCC Recurrence After Ablation Therapy
- PMID: 34094938
- PMCID: PMC8176857
- DOI: 10.3389/fonc.2021.649682
Preoperative Gadoxetic Acid-Enhanced MRI Based Nomogram Improves Prediction of Early HCC Recurrence After Ablation Therapy
Abstract
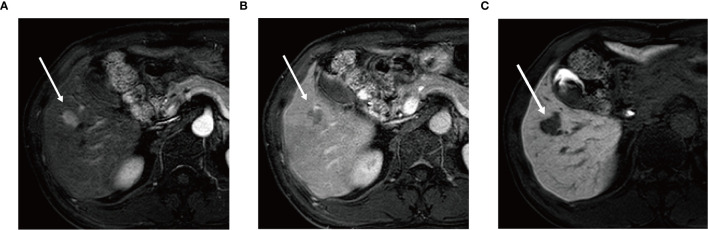
Purpose: This study aimed to identify preoperative gadoxetic acid-enhanced MRI features and establish a nomogram for predicting early recurrence (≤ 2 years) of hepatocellular carcinoma (HCC) after ablation therapy.
Methods: A total of 160 patients who underwent gadoxetic acid-enhanced MRI and ablation HCC therapy from January 2015 to June 2018, were included retrospectively and divided into a training cohort (n = 112) and a validation cohort (n = 48). Independent clinical risk factors and gadoxetic acid-enhanced MRI features associated with early recurrence were identified by univariate and multivariate logistic regression analysis and used for construction of a nomogram. The performance of the nomogram was evaluated by discrimination, calibration, and clinical utility.
Results: Alpha-fetoprotein (AFP) level, tumor number, arterial peritumoral enhancement, satellite nodule and peritumoral hypointensity at hepatobiliary phases in the training cohort were identified as independent risk factors for early recurrence after ablation. A new nomogram that was constructed with these five features showed an area under the curve (AUC) of 0.843 (95%CI 0.771-0.916) and 0.835 (95%CI 0.713-0.956) in the training and validation cohort, respectively. The calibration curve and decision curve analysis (DCA) suggested that the nomogram had good consistency and clinical utility.
Conclusions: A new nomogram that was constructed using four preoperative gadoxetic acid-enhanced MRI features and serum AFP level can predict the risk of early HCC recurrence after ablation therapy with AUC up to 0.843. The strong performance of this nomogram may help hepatologists to categorize patients' recurrent risk to guide selecting treatment options and improve postoperative management.
Keywords: ablation technique; early recurrence; hepatocellular carcinoma; magnetic resonance imaging; nomogram; prediction.
Copyright © 2021 Hu, Song, Zhang, Dai, Tang, Li, Liao, Zhou, Xu, Zhang and Zhou.
Conflict of interest statement
Y-YZ is the founder and CSO of HBVtech. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






Similar articles
-
Gadoxetic acid-enhanced MRI with a focus on LI-RADS v2018 imaging features predicts the prognosis after radiofrequency ablation in small hepatocellular carcinoma.Front Oncol. 2023 Feb 2;13:975216. doi: 10.3389/fonc.2023.975216. eCollection 2023. Front Oncol. 2023. PMID: 36816925 Free PMC article.
-
Hepatobiliary Phase Features of Preoperative Gadobenate-Enhanced MR can Predict Early Recurrence of Hepatocellular Carcinoma in Patients Who Underwent Anatomical Hepatectomy.Front Oncol. 2022 Aug 3;12:862967. doi: 10.3389/fonc.2022.862967. eCollection 2022. Front Oncol. 2022. PMID: 35992871 Free PMC article.
-
Prediction early recurrence of hepatocellular carcinoma after hepatectomy using gadoxetic acid-enhanced MRI and IVIM.Eur J Radiol Open. 2025 Mar 15;14:100643. doi: 10.1016/j.ejro.2025.100643. eCollection 2025 Jun. Eur J Radiol Open. 2025. PMID: 40166482 Free PMC article.
-
Radiomics nomogram for prediction of glypican-3 positive hepatocellular carcinoma based on hepatobiliary phase imaging.Front Oncol. 2023 Sep 29;13:1209814. doi: 10.3389/fonc.2023.1209814. eCollection 2023. Front Oncol. 2023. PMID: 37841420 Free PMC article.
-
A Radiomics Nomogram for Preoperative Prediction of Microvascular Invasion in Hepatocellular Carcinoma.Liver Cancer. 2019 Oct;8(5):373-386. doi: 10.1159/000494099. Epub 2018 Nov 27. Liver Cancer. 2019. PMID: 31768346 Free PMC article.
Cited by
-
The Role of Radiomics and AI Technologies in the Segmentation, Detection, and Management of Hepatocellular Carcinoma.Cancers (Basel). 2022 Dec 12;14(24):6123. doi: 10.3390/cancers14246123. Cancers (Basel). 2022. PMID: 36551606 Free PMC article. Review.
-
Clinical and Imaging-Based Prognostic Models for Recurrence and Local Tumor Progression Following Thermal Ablation of Hepatocellular Carcinoma: A Systematic Review.Cancers (Basel). 2025 Aug 14;17(16):2656. doi: 10.3390/cancers17162656. Cancers (Basel). 2025. PMID: 40867285 Free PMC article. Review.
-
Gadoxetic acid-enhanced MRI with a focus on LI-RADS v2018 imaging features predicts the prognosis after radiofrequency ablation in small hepatocellular carcinoma.Front Oncol. 2023 Feb 2;13:975216. doi: 10.3389/fonc.2023.975216. eCollection 2023. Front Oncol. 2023. PMID: 36816925 Free PMC article.
-
Hepatobiliary Phase Features of Preoperative Gadobenate-Enhanced MR can Predict Early Recurrence of Hepatocellular Carcinoma in Patients Who Underwent Anatomical Hepatectomy.Front Oncol. 2022 Aug 3;12:862967. doi: 10.3389/fonc.2022.862967. eCollection 2022. Front Oncol. 2022. PMID: 35992871 Free PMC article.
-
Preparation of NIR-Responsive Gold Nanocages as Efficient Carrier for Controlling Release of EGCG in Anticancer Application.Front Chem. 2022 Jun 2;10:926002. doi: 10.3389/fchem.2022.926002. eCollection 2022. Front Chem. 2022. PMID: 35720982 Free PMC article.
References
-
- Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, Brenner H, et al. . Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol (2017) 3(4):524–48. 10.1001/jamaoncol.2016.5688 - DOI - PMC - PubMed
-
- Vietti VN, Duran R, Guiu B, Cercueil JP, Aube C, Digklia A, et al. . Efficacy of Microwave Ablation Versus Radiofrequency Ablation for the Treatment of Hepatocellular Carcinoma in Patients With Chronic Liver Disease: A Randomised Controlled Phase 2 Trial. Lancet Gastroenterol Hepatol (2018) 3(5):317–25. 10.1016/S2468-1253(18)30029-3 - DOI - PubMed
LinkOut - more resources
Full Text Sources