

Prophylactic Intra-Peritoneal Drainage After Pancreatic Resection: An Updated Meta-Analysis
- PMID: 34094952
- PMCID: PMC8172774
- DOI: 10.3389/fonc.2021.658829
Prophylactic Intra-Peritoneal Drainage After Pancreatic Resection: An Updated Meta-Analysis
Abstract
Introduction: Prophylactic intra-peritoneal drainage has been considered to be an effective measure to reduce postoperative complications after pancreatectomy. However, routinely placed drainage during abdominal surgery may be unnecessary or even harmful to some patients, due to the possibility of increasing complications. And there is still controversy about the prophylactic intra-peritoneal drainage after pancreatectomy. This meta-analysis aimed to analyze the incidence of complications after either pancreaticoduodenectomy (PD) or distal pancreatectomy (DP) in the drain group and no-drain group.
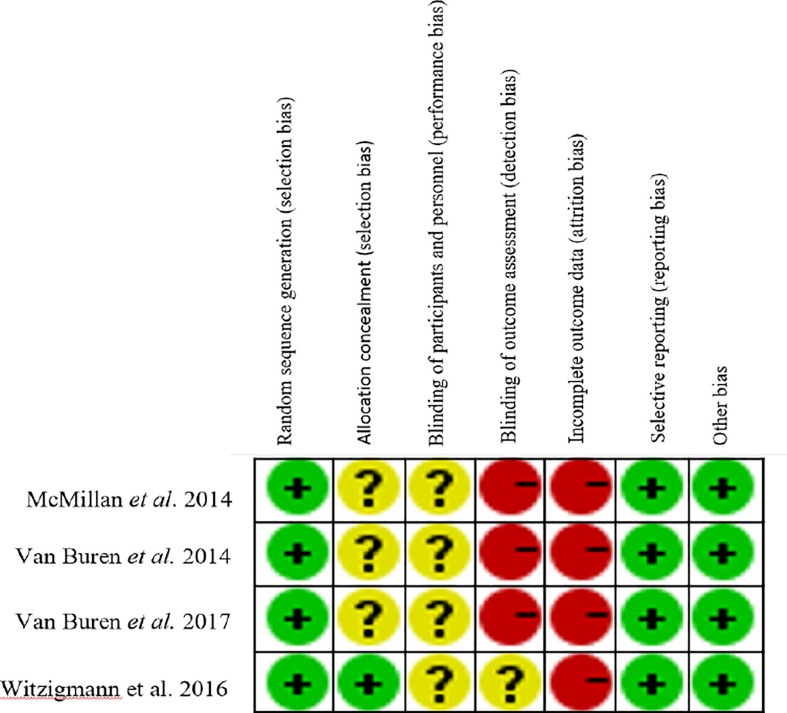
Methods: Data were retrieved from four electronic databases PubMed, EMBASE, the Cochrane Library and Web of Science up to December 2020, including the outcomes of individual treatment after PD and DP, mortality, morbidity, clinically relevant postoperative pancreatic fistula (CR-POPF), bile leak, wound infection, postoperative hemorrhage, delayed gastric emptying (DGE), intra-abdominal abscess, reoperation, intervened radiology (IR), and readmission. Cochrane Collaboration Handbook and the criteria of the Newcastle-Ottawa scale were used to assess the quality of studies included.
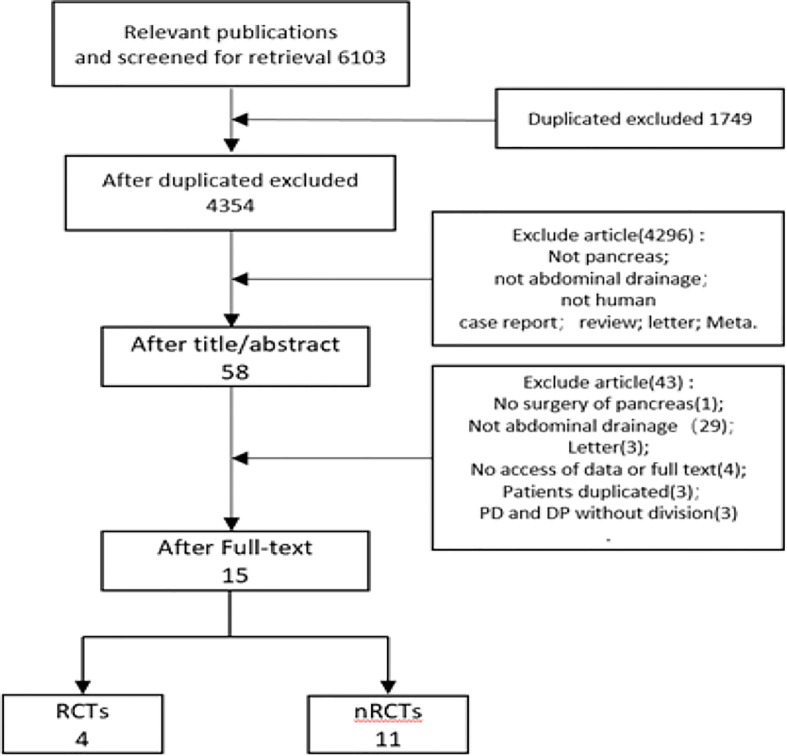
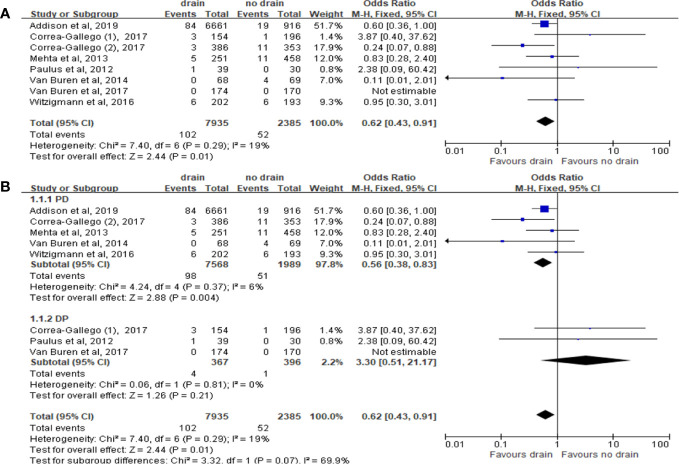
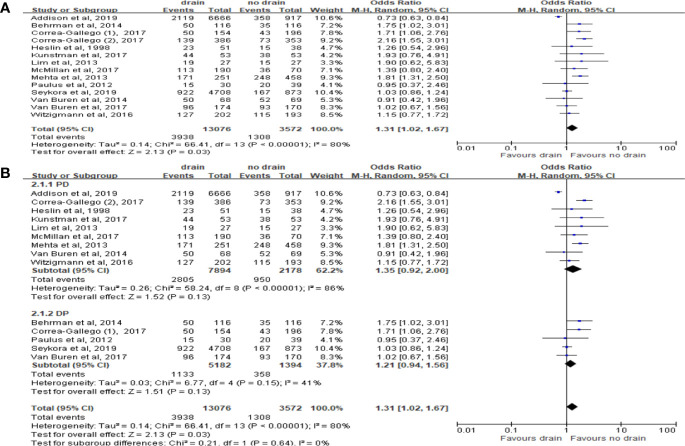
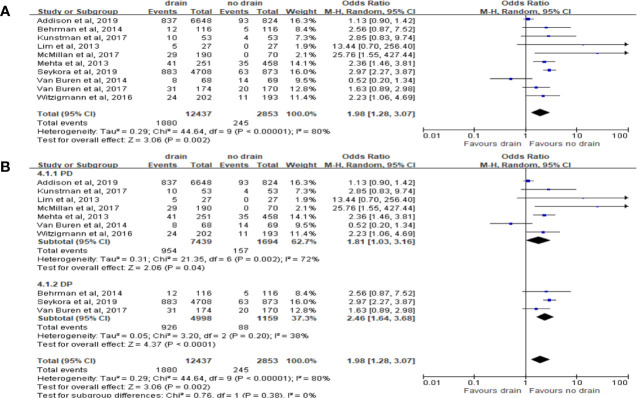
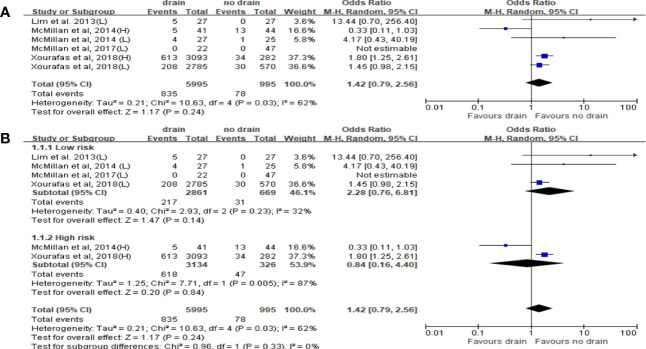
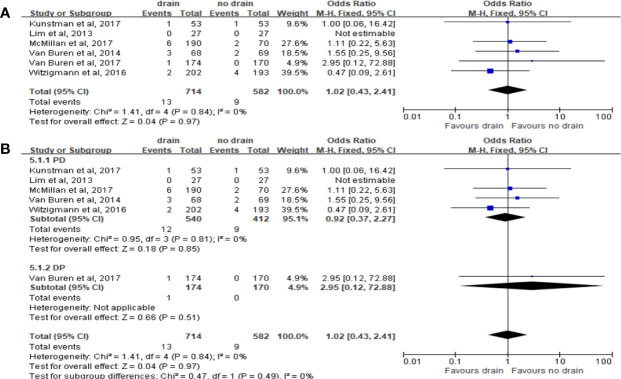
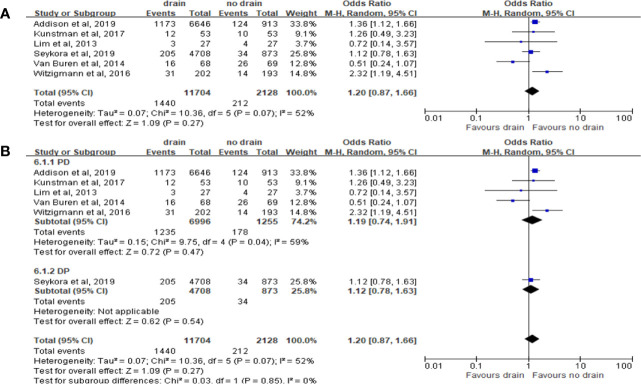
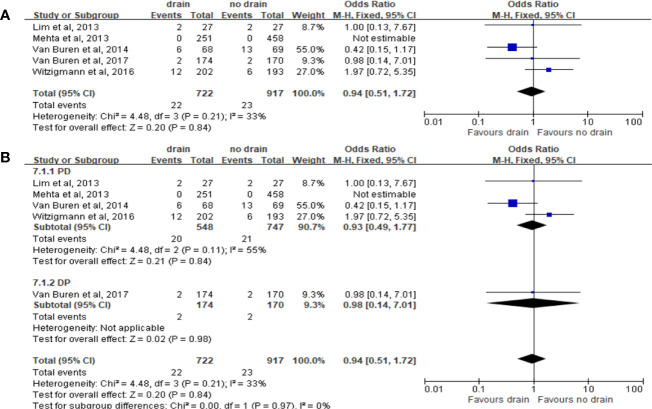
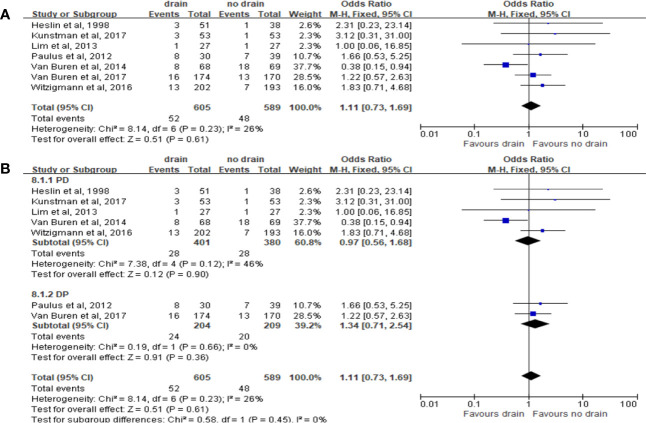
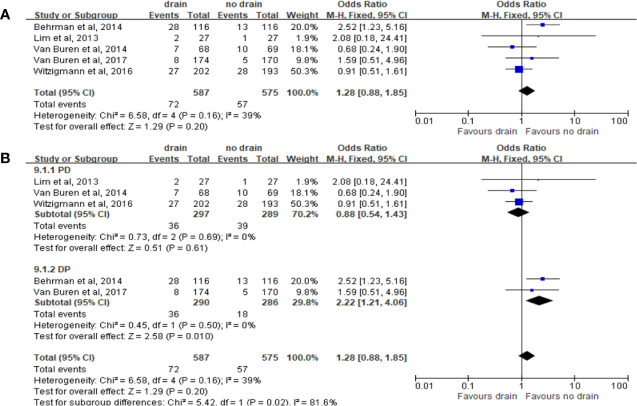
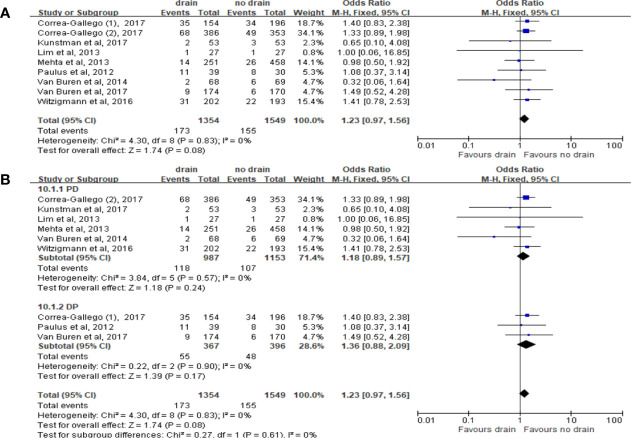
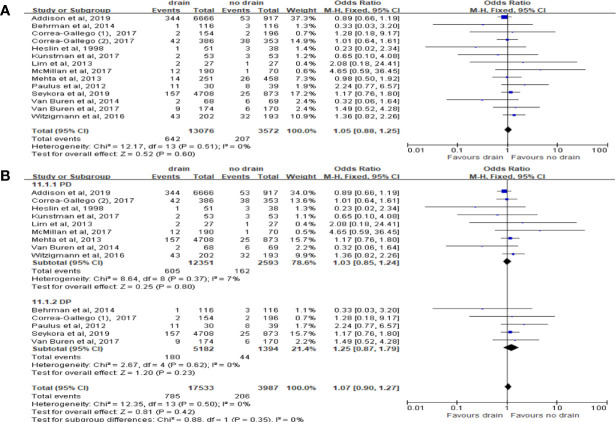
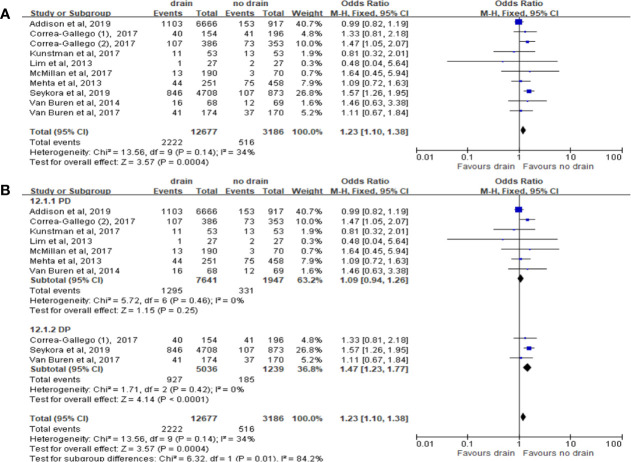
Results: We included 15 studies after strict screening. 13 studies with 16,648 patients were analyzed to assess the effect of drain placement on patients with different surgery procedures, and 4 studies with 6,990 patients were analyzed to assess the effect of drain placement on patients with different fistula risk. For patients undergoing PD, the drain group had lower mortality but higher rate of CR-POPF than the no-drain group. For patients undergoing DP, the drain group had higher rates of CR-POPF, wound infection and readmission. There were no significant differences in bile leak, hemorrhage, DGE, intra-abdominal abscess, and IR in either overall or each subgroup. For Low-risk subgroup, the rates of hemorrhage, DGE and morbidity were higher after drainage. For High-risk subgroup, the rate of hemorrhage was higher while the rates of reoperation and morbidity were lower in the drain group.
Conclusions: Intraperitoneal drainage may benefit some patients undergoing PD, especially those with high pancreatic fistula risk. For DP, current evidences suggest that routine drainage might not benefit patients, but no clear conclusions can be drawn because of the study limitations.
Keywords: distal pancreatectomy; intra-peritoneal drainage; meta-analysis; pancreatic resection; pancreaticoduodenectomy.
Copyright © 2021 Liu, Chen, Chu, Liu, Yang and Tian.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Early vs late drain removal after pancreatic resection-a systematic review and meta-analysis.Langenbecks Arch Surg. 2023 Aug 17;408(1):317. doi: 10.1007/s00423-023-03053-6. Langenbecks Arch Surg. 2023. PMID: 37587225
-
Peritoneal drainage or no drainage after pancreaticoduodenectomy and/or distal pancreatectomy: a meta-analysis and systematic review.Surg Endosc. 2020 Nov;34(11):4991-5005. doi: 10.1007/s00464-019-07293-w. Epub 2019 Dec 6. Surg Endosc. 2020. PMID: 31811457
-
Prophylactic abdominal drainage or no drainage after distal pancreatectomy (PANDORINA): a binational multicenter randomized controlled trial.Trials. 2022 Sep 24;23(1):809. doi: 10.1186/s13063-022-06736-5. Trials. 2022. PMID: 36153559 Free PMC article. Clinical Trial.
-
Early Drain Removal Versus Routine Drain Removal After Pancreaticoduodenectomy and/or Distal Pancreatectomy: A Meta-Analysis and Systematic Review.Dig Dis Sci. 2024 Sep;69(9):3450-3465. doi: 10.1007/s10620-024-08547-x. Epub 2024 Jul 23. Dig Dis Sci. 2024. PMID: 39044014
-
Surgical drain placement in distal pancreatectomy is associated with an increased incidence of postoperative pancreatic fistula and higher readmission rates.J Surg Oncol. 2020 Sep;122(4):723-728. doi: 10.1002/jso.26072. Epub 2020 Jul 2. J Surg Oncol. 2020. PMID: 32614999 Free PMC article.
Cited by
-
[Anastomotic leakage in hepato-pancreato-biliary surgery].Chirurgie (Heidelb). 2024 Nov;95(11):887-894. doi: 10.1007/s00104-024-02176-w. Epub 2024 Sep 28. Chirurgie (Heidelb). 2024. PMID: 39340543 German.
-
The image-based preoperative fistula risk score (preFRS) predicts postoperative pancreatic fistula in patients undergoing pancreatic head resection.Sci Rep. 2022 Mar 8;12(1):4064. doi: 10.1038/s41598-022-07970-2. Sci Rep. 2022. PMID: 35260701 Free PMC article.
-
Early vs late drain removal after pancreatic resection-a systematic review and meta-analysis.Langenbecks Arch Surg. 2023 Aug 17;408(1):317. doi: 10.1007/s00423-023-03053-6. Langenbecks Arch Surg. 2023. PMID: 37587225
-
Prophylactic drainage versus non-drainage following gastric cancer surgery: a meta-analysis of randomized controlled trials and observational studies.World J Surg Oncol. 2023 Jun 3;21(1):166. doi: 10.1186/s12957-023-03054-1. World J Surg Oncol. 2023. PMID: 37270519 Free PMC article.
-
The role of clinically relevant intra-abdominal collections after pancreaticoduodenectomy : Clinical impact and predictors. A retrospective analysis from a European tertiary centre.Langenbecks Arch Surg. 2023 Dec 28;409(1):21. doi: 10.1007/s00423-023-03200-z. Langenbecks Arch Surg. 2023. PMID: 38151676 Free PMC article.
References
-
- Jilesen AP, van Eijck CH, in’t Hof KH, van Dieren S, Gouma DJ, van Dijkum EJ. Postoperative Complications, in-Hospital Mortality and 5-Year Survival After Surgical Resection for Patients With a Pancreatic Neuroendocrine Tumor: A Systematic Review. World J Surg (2016) 40:729–48. 10.1007/s00268-015-3328-6 - DOI - PMC - PubMed
-
- Pedrazzoli S. Pancreatoduodenectomy (PD) and Postoperative Pancreatic Fistula (POPF): A Systematic Review and Analysis of the POPF-related Mortality Rate in 60,739 Patients Retrieved From the English Literature Published Between 1990 and 2015. Med (Baltimore) (2017) 96:e6858. 10.1097/MD.0000000000006858 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources