

PSA Density Help to Identify Patients With Elevated PSA Due to Prostate Cancer Rather Than Intraprostatic Inflammation: A Prospective Single Center Study
- PMID: 34094990
- PMCID: PMC8173030
- DOI: 10.3389/fonc.2021.693684
PSA Density Help to Identify Patients With Elevated PSA Due to Prostate Cancer Rather Than Intraprostatic Inflammation: A Prospective Single Center Study
Abstract
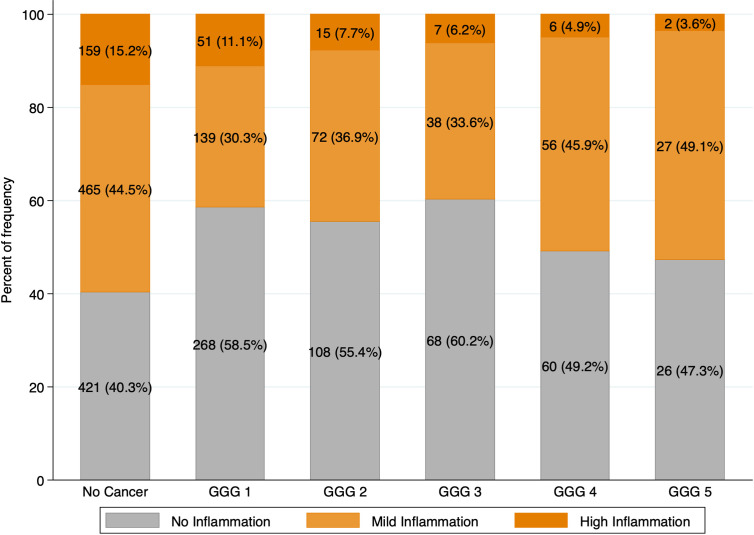
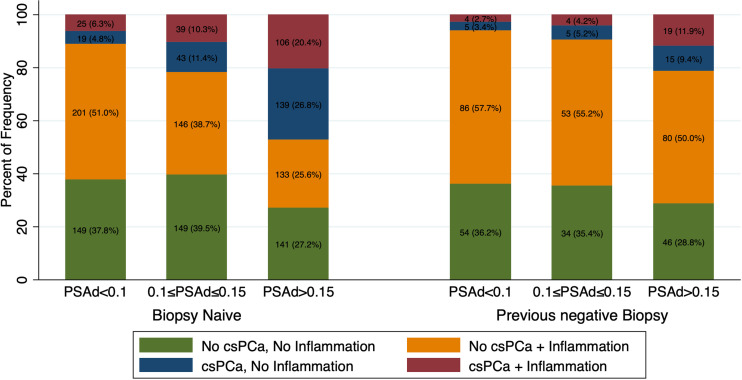
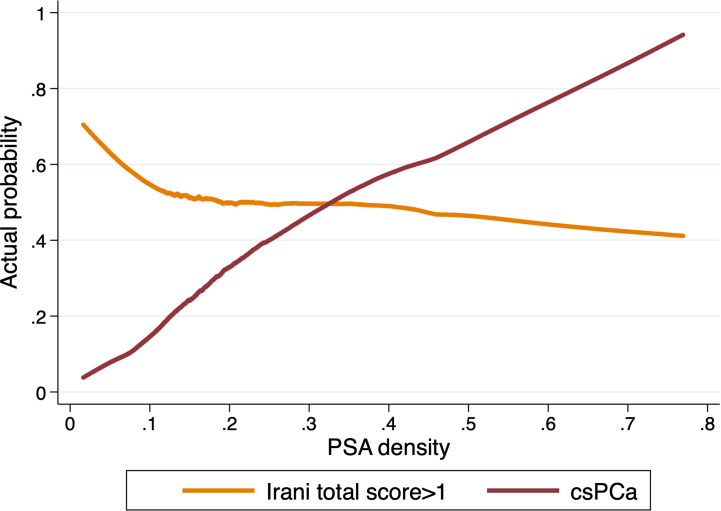
The association between PSA density, prostate cancer (PCa) and BPH is well established. The aim of the present study was to establish whether PSA density can be used as a reliable parameter to predict csPCa and to determine its optimal cutoff to exclude increased PSA levels due to intraprostatic inflammation. This is a large prospective single-center, observational study evaluating the role of PSA density in the discrimination between intraprostatic inflammation and clinically significant PCa (csPCa). Patients with PSA ≥ 4 ng/ml and/or positive digito-rectal examination (DRE) and scheduled for prostate biopsy were enrolled. Prostatic inflammation (PI) was assessed and graded using the Irani Scores. Multivariable binary logistic regression analysis was used to assess if PSA density was associated with clinically significant PCa (csPCa) rather than prostatic inflammation. A total of 1988 patients met the inclusion criteria. Any PCa and csPCa rates were 47% and 24% respectively. In the group without csPCa, patients with prostatic inflammation had a higher PSA (6.0 vs 5.0 ng/ml; p=0.0003), higher prostate volume (58 vs 52 cc; p<0.0001), were more likely to have a previous negative biopsy (29% vs 21%; p=0.0005) and a negative DRE (70% vs 65%; p=0.023) but no difference in PSA density (0.1 vs 0.11; p=0.2). Conversely in the group with csPCa, patients with prostatic inflammation had a higher prostate volume (43 vs 40 cc; p=0.007) but no difference in the other clinical parameters. At multivariable analysis adjusting for age, biopsy history, DRE and prostate volume, PSA density emerged as a strong predictor of csPCA but was not associated with prostatic inflammation. The optimal cutoffs of PSA density to diagnose csPCa and rule out the presence of prostatic inflammation in patients with an elevated PSA (>4 ng/ml) were 0.10 ng/ml2 in biopsy naïve patients and 0.15 ng/ml2 in patients with a previous negative biopsy. PSA density rather than PSA, should be used to evaluate patients at risk of prostate cancer who may need additional testing or prostate biopsy. This readily available parameter can potentially identify men who do not have PCa but have an elevated PSA secondary to benign conditions.
Keywords: Irani score; PSA; PSA density; prostate cancer; prostate inflammation.
Copyright © 2021 Bruno, Falagario, d’Altilia, Recchia, Mancini, Selvaggio, Sanguedolce, Del Giudice, Maggi, Ferro, Porreca, Sciarra, De Berardinis, Bettocchi, Busetto, Cormio and Carrieri.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Mottet N, van den Bergh RCN, Briers E, Cornford P, De Santis M, Fanti S, et al. . Eau - ESTRO - ESUR - SIOG Guidelines on Prostate Cancer 2020. In: . European Association of Urology Guidelines. 2020 Edition. Arnhem, The Netherlands: European Association of Urology Guidelines Office; (2020). presented at the EAU Annual Congress Amsterdam 2020.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous