

Disease-associated reference intervals for twenty laboratory tests in patients with rheumatoid arthritis, Crohn's disease or ulcerative colitis
- PMID: 34095413
- PMCID: PMC8145736
- DOI: 10.1016/j.plabm.2021.e00225
Disease-associated reference intervals for twenty laboratory tests in patients with rheumatoid arthritis, Crohn's disease or ulcerative colitis
Abstract
Background: Population based reference intervals are fundamental for interpreting results for quantitative laboratory tests. In patients with a specific chronic disorder, however, results of various tests may regularly be different than in healthy individuals. Health-associated reference intervals may therefore have limited value in such patients. Instead, disease-associated reference intervals may be useful, as they describe the results distribution in populations resembling the specific patients. Few disease-associated reference intervals are available in the literature. The aim of this study was to estimate reference intervals for common laboratory tests for patient populations with rheumatoid arthritis, Crohn's disease or ulcerative colitis without significant comorbidity, using a novel algorithm.
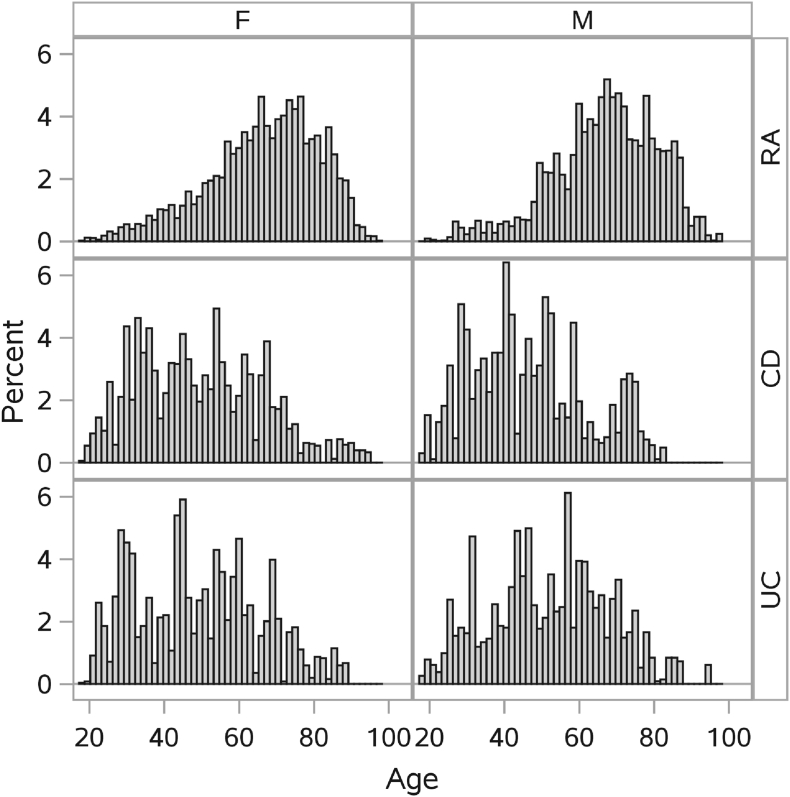
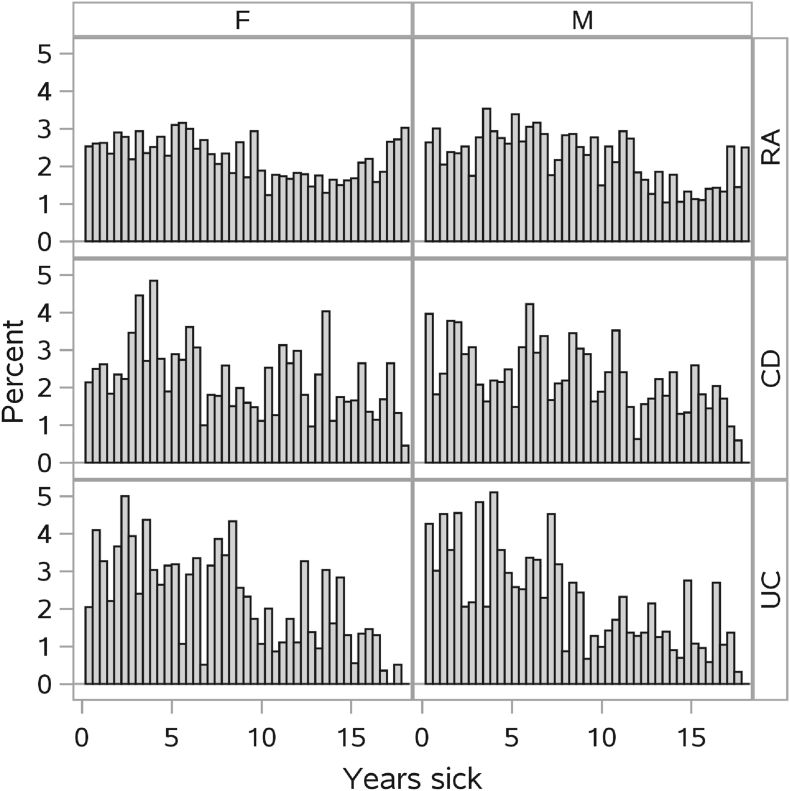
Material and methods: Laboratory test results and hospital discharge diagnoses were collected for relevant patients. An algorithm was developed to identify discharge diagnoses significantly associated with high or low results for specific tests. After excluding patients with such diagnoses, reference intervals were estimated, representing results distributions in patients with each of the specific chronic disorders, but without significant comorbidity.
Results: Disease-associated reference intervals were estimated for 20 common laboratory tests. Most of the estimated reference limits were significantly different from corresponding health-associated reference limits. Thirty percent of the estimated reference intervals were different from estimates based on crude patient populations, indicating that the algorithm applied managed to exclude patients with relevant comorbidity.
Conclusion: Disease-associated reference intervals could be estimated for a number of tests in patients with rheumatoid arthritis, ulcerative colitis or Crohn's disease using a highly automated algorithm based on routinely recorded patient data.
Keywords: Crohn’s disease; Reference intervals; Rheumatoid arthritis; Ulcerative colitis.
© 2021 The Authors.
Conflict of interest statement
None.
Figures

References
-
- Solberg H.E. International federation of clinical chemistry (IFCC), scientific committee, clinical section, expert panel on theory of reference values, and international committee for standardization in haematology (ICSH), standing committee on reference values. Approved recommendation (1986) on the theory of reference values. Part 1. The concept of reference values. J. Clin. Chem. Clin. Biochem. 1987;25(5):337–342. - PubMed
-
- Horowitz G., Jones G.R.D. Establishment and Use of Reference Intervals. In: Rifai N., Horvath A.R., Wittwer C.T., editors. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics. sixth ed. Elsevier Saunders; 2018. pp. 170–194. ISBN: 978-0-323-35921-4.
-
- Adeli K., Ceriotti F., Nieuwesteeg M. Reference Information for the Clinical Laboratory. In: Burtis C.A., Ashwood E.R., Bruns D.E., editors. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics. sixth ed. Elsevier Saunders; 2018. pp. 1745–1818. ISBN: 978-0-323-35921-4.
-
- Solberg H.E., PetitClerc C. International federation of clinical chemistry (IFCC), scientific committee, clinical section, expert panel on theory of reference values. Approved recommendation (1988) on the theory of reference values. Part 3. Preparation of individuals and collection of specimens for the production of reference values. J. Clin. Chem. Clin. Biochem. 1988;26(9):593–598. - PubMed
-
- Defining C.L.S.I. third ed. 2008. Establishing, and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline; p. 37. (CLSI Document C28-A3c).
LinkOut - more resources
Full Text Sources
