

The Vanishing Adrenal Glands: A Transient Regression of Adrenal Lymphoma After a Single Dose of 1 mg Dexamethasone
- PMID: 34095465
- PMCID: PMC8053686
- DOI: 10.1016/j.aace.2020.11.022
The Vanishing Adrenal Glands: A Transient Regression of Adrenal Lymphoma After a Single Dose of 1 mg Dexamethasone
Abstract
Objective: Dexamethasone is a known treatment for lymphoma, but the potency and rapidity of its effect have not been recognized. We present a case of bilateral adrenal lymphoma that significantly reduced in size after a single dose of dexamethasone.
Methods: We present the clinical course and investigations, including adrenocorticotropic hormone, cortisol, short synacthen test, computed tomography (CT), and adrenal biopsy results.
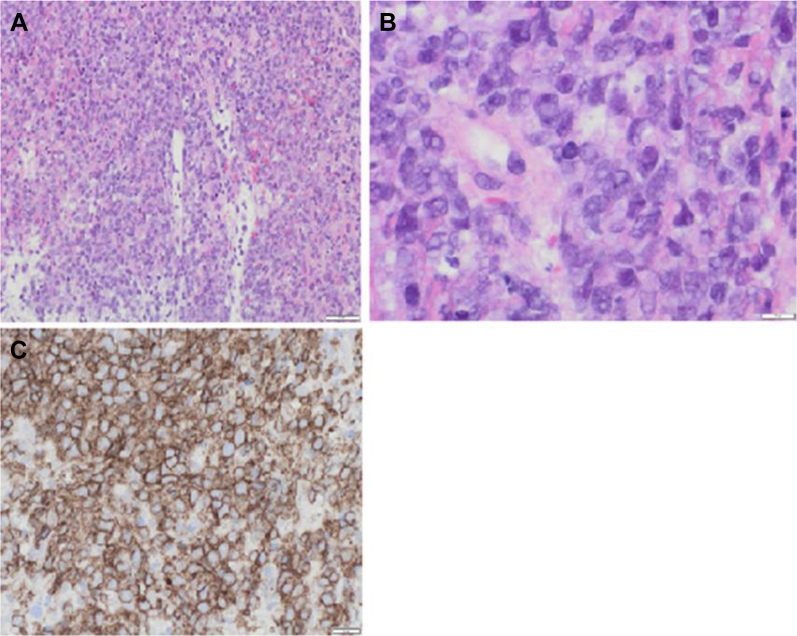
Results: A 52-year-old man had a fall and was incidentally found to have bilateral adrenal masses (left, 6 cm; right, 5 cm) on CT. His adrenal function tests included plasma metanephrines (normetanephrine, 830 pmol/L [normal, <1180]; metanephrine, <100 pmol/L [<510]; 3-methoxytyramine, <100 pmol/L [<180]); aldosterone, 270 pmol/L( 90-700); and random cortisol, 230 nmol/L (160-550). An overnight dexamethasone suppression test with 1 mg of dexamethasone showed cortisol of <28 nmol/L (0-50). A repeat CT scan 8 days thereafter showed adrenal masses of 4.5 and 3.5 cm on the left and right, respectively. He had a follow-up CT scan 3 months later that showed adrenal lesions measuring 8 cm (left) and 9 cm (right). He subsequently presented with fatigue and dizziness. Morning cortisol of 201 nmol/L (160-550) with adrenocorticotropic hormone of 216 ng/L (10-30) indicated primary adrenal insufficiency. Mineralocorticoid and glucocorticoid replacement therapy commenced. An adrenal biopsy showed abnormal enlarged B cells, consistent with a diagnosis of diffuse large B-cell lymphoma.
Conclusion: A diagnosis of lymphoma should be considered when adrenal lesions shrink following even a single low dose of dexamethasone administered as a part of a diagnostic test.
Keywords: ACTH, adrenocorticotropic hormone; CT, computed tomography; DLBCL, diffuse large B-cell lymphoma; ONDST, overnight dexamethasone suppression test; PAI, primary adrenal insufficiency; PET, positron emission tomography; SST, short synacthen test; adrenal; adrenal cancer; adrenal insufficiency.
© 2020 AACE. Published by Elsevier Inc.
Figures

Similar articles
-
ACTH following overnight dexamethasone suppression can be used in the verification of autonomous cortisol secretion in patients with adrenal incidentalomas.Clin Endocrinol (Oxf). 2021 Feb;94(2):168-175. doi: 10.1111/cen.14357. Epub 2020 Nov 15. Clin Endocrinol (Oxf). 2021. PMID: 33108675
-
Primary Adrenal Lymphomas with Cushing's Syndrome: Two Cases with Evidence of Endogeneous Cortisol Production by the Neoplastic Lymphoid Cells.J Clin Med. 2023 Jul 31;12(15):5032. doi: 10.3390/jcm12155032. J Clin Med. 2023. PMID: 37568434 Free PMC article.
-
Nonseminomatous Germ-Cell Tumor Presenting as Bilateral Adrenal Masses.AACE Clin Case Rep. 2020 Dec 28;7(1):43-46. doi: 10.1016/j.aace.2020.11.011. eCollection 2021 Jan-Feb. AACE Clin Case Rep. 2020. PMID: 33851019 Free PMC article.
-
Primary adrenal non-Hodgkin lymphoma: a case report and review of the literature.J Med Case Rep. 2017 Apr 15;11(1):108. doi: 10.1186/s13256-017-1271-x. J Med Case Rep. 2017. PMID: 28410600 Free PMC article. Review.
-
[Primary adrenal lymphoma: a case report and literature review in Japan].Rinsho Ketsueki. 2002 Sep;43(9):851-6. Rinsho Ketsueki. 2002. PMID: 12412291 Review. Japanese.
References
-
- Günaydin A., Er U., Acuduman A., Sabuncuoğlu H., Oztürk E. Diagnostic and surgical pitfalls of an unusual primary central nervous system lymphoma. Turk Neurosurg. 2007;17(2):129–133. - PubMed
-
- Farquhar D., Sobanko J., Williams K., Newman J.G. A vanishing lymphoma in the cheek. ORL J Otorhinolaryngol Relat Spec. 2014;76(4):189–192. - PubMed
-
- Rashidi A., Fisher S.I. Primary adrenal lymphoma: a systematic review. Ann Hematol. 2013;92(12):1583–1593. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous