

Cushing's Disease as a Result of Two ACTH-Secreting Pituitary Tumors
- PMID: 34095475
- PMCID: PMC8053624
- DOI: 10.1016/j.aace.2020.12.002
Cushing's Disease as a Result of Two ACTH-Secreting Pituitary Tumors
Abstract
Objective: Our objective is to present a case of Cushing's disease (CD) with 2 adrenocorticotropic hormone (ACTH)-secreting pituitary tumors. Multiple monohormonal pituitary tumors are rare. This case supports a consideration of repeat transsphenoidal surgery (TSS) in patients with initial surgical failure.
Methods: Salivary, 24-h urine, serum cortisol testing, and magnetic resonance imaging (MRI) were used to diagnose CD. Treatment included TSS and postoperative hydrocortisone.
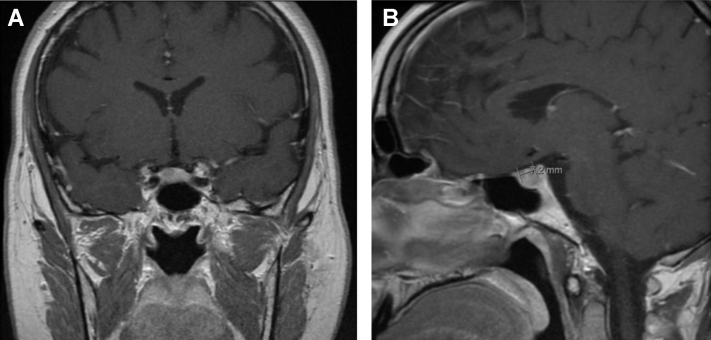
Results: A 36-year-old woman followed for hypothyroidism presented with a new left supraclavicular fossa swelling and underwent Cushing's syndrome screening. The levels of late-night salivary cortisol were 0.636 and 0.316 μg/dL, 24-h urine cortisol was 162 μg/24 h, cortisol after 1-mg dexamethasone suppression was 14.0 μg/dL, and serum morning cortisol was 26.4 μg/dL with ACTH of 66.7 pg/mL. A 7-mm hypoenhancing anterior pituitary lesion was noted on pituitary MRI. The cortisol level was 2.7 μg/dL after an 8-mg dexamethasone suppression. She underwent TSS, and her histopathology read as pituitary adenoma staining positive for ACTH. No residual tumor was seen intraoperatively. Postoperative morning serum cortisol was 17.9 μg/dL, and ACTH level was 79 pg/mL. Repeat TSS revealed a second adenoma previously unseen on MRI, which also stained positive for ACTH. Postoperative morning cortisol was 0.7 μg/dL, and ACTH was <9 pg/mL. Hydrocortisone, which was started for her central adrenal insufficiency, was tapered and stopped 1 year postoperatively. Late-night salivary cortisol levels were 0.016 and 0.012 μg/dL.
Conclusion: We conclude that surgical failure in CD after initial TSS should warrant the consideration of a second ACTH-secreting pituitary adenoma and possible repeat TSS.
Keywords: ACTH, adrenocorticotropic hormone; ACTH-secreting pituitary adenoma; CD, Cushing’s disease; Cushing’s syndrome; MRI, magnetic resonance imaging; TSS, transsphenoidal surgery; pituitary tumors.
© 2020 AACE. Published by Elsevier Inc.
Figures

References
-
- Burke W.T., Penn D.L., Repetti C.S. Outcomes after repeat transsphenoidal surgery for recurrent Cushing disease: updated. Neurosurgery. 2019;85(6):E1030–E1036. - PubMed
-
- Rubinstein G., Ossald A., Zopp S. Therapeutic options after surgical failure in Cushing’s disease: a critical review. Best Pract Res Clin Endocrinol Metab. 2019;33(2):101270. - PubMed
-
- Faggiano A., Pivonello R., Melis D. Nephrolithiasis in Cushing’s disease: prevalence, etiopathogenesis, and modification after disease cure. J Clin Endocrinol Metab. 2003;88(5):2076–2080. - PubMed
Publication types
LinkOut - more resources
Full Text Sources