

Immune Thrombocytopenia: Recent Advances in Pathogenesis and Treatments
- PMID: 34095758
- PMCID: PMC8171374
- DOI: 10.1097/HS9.0000000000000574
Immune Thrombocytopenia: Recent Advances in Pathogenesis and Treatments
Abstract
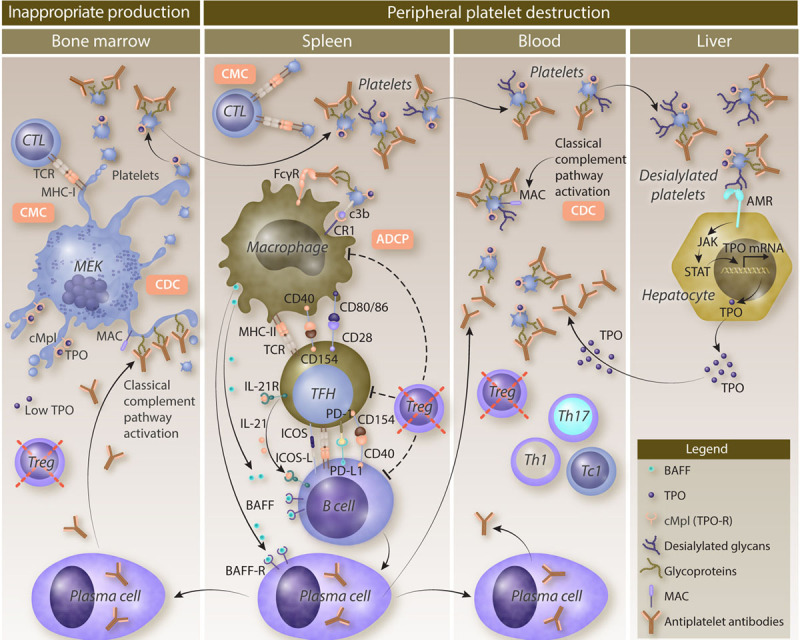
Immune thrombocytopenia (ITP) is a rare autoimmune disease due to both a peripheral destruction of platelets and an inappropriate bone marrow production. Although the primary triggering factors of ITP remain unknown, a loss of immune tolerance-mostly represented by a regulatory T-cell defect-allows T follicular helper cells to stimulate autoreactive splenic B cells that differentiate into antiplatelet antibody-producing plasma cells. Glycoprotein IIb/IIIa is the main target of antiplatelet antibodies leading to platelet phagocytosis by splenic macrophages, through interactions with Fc gamma receptors (FcγRs) and complement receptors. This allows macrophages to activate autoreactive T cells by their antigen-presenting functions. Moreover, the activation of the classical complement pathway participates to platelet opsonization and also to their destruction by complement-dependent cytotoxicity. Platelet destruction is also mediated by a FcγR-independent pathway, involving platelet desialylation that favors their binding to the Ashwell-Morell receptor and their clearance in the liver. Cytotoxic T cells also contribute to ITP pathogenesis by mediating cytotoxicity against megakaryocytes and peripheral platelets. The deficient megakaryopoiesis resulting from both the humoral and the cytotoxic immune responses is sustained by inappropriate levels of thrombopoietin, the major growth factor of megakaryocytes. The better understanding of ITP pathogenesis has provided important therapeutic advances. B cell-targeting therapies and thrombopoietin-receptor agonists (TPO-RAs) have been used for years. New emerging therapeutic strategies that inhibit FcγR signaling, the neonatal Fc receptor or the classical complement pathway, will deeply modify the management of ITP in the near future.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Figures
References
-
- Moulis G, Palmaro A, Montastruc JL, et al. Epidemiology of incident immune thrombocytopenia: a nationwide population-based study in France. Blood. 2014; 124:3308–3315. - PubMed
-
- Audia S, Mahévas M, Samson M, et al. Pathogenesis of immune thrombocytopenia. Autoimmun Rev. 2017; 16:620–632. - PubMed
-
- Audia S, Moulinet T, Ciudad-Bonté M, et al. Altered distribution and function of splenic innate lymphoid cells in adult chronic immune thrombocytopenia. J Autoimmun. 2018; 93:139–144. - PubMed
-
- Michel M, Lega JC, Terriou L. [Secondary ITP in adults]. Rev Med Interne. 2021; 42:50–57. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources