

Laboratory trends, hyperinflammation, and clinical outcomes for patients with a systemic rheumatic disease admitted to hospital for COVID-19: a retrospective, comparative cohort study
- PMID: 34095857
- PMCID: PMC8163294
- DOI: 10.1016/S2665-9913(21)00140-5
Laboratory trends, hyperinflammation, and clinical outcomes for patients with a systemic rheumatic disease admitted to hospital for COVID-19: a retrospective, comparative cohort study
Abstract
Background: COVID-19 can induce a hyperinflammatory state, which might lead to poor clinical outcomes. We aimed to assess whether patients with a systemic rheumatic disease might be at increased risk for hyperinflammation and respiratory failure from COVID-19.
Methods: We did a retrospective, comparative cohort study of patients aged 18 years or older admitted to hospital with PCR-confirmed COVID-19 at Mass General Brigham (Boston, USA). We identified patients by a search of electronic health records and matched patients with a systemic rheumatic disease 1:5 to comparators. We compared individual laboratory results by case status and extracted laboratory results and COVID-19 outcomes for each participant. We calculated the COVID-19-associated hyperinflammation score (cHIS), a composite of six domains (a score of ≥2 indicating hyperinflammation) and used logistic regression to estimate odds ratios (ORs) for COVID-19 outcomes by hyperinflammation and case status.
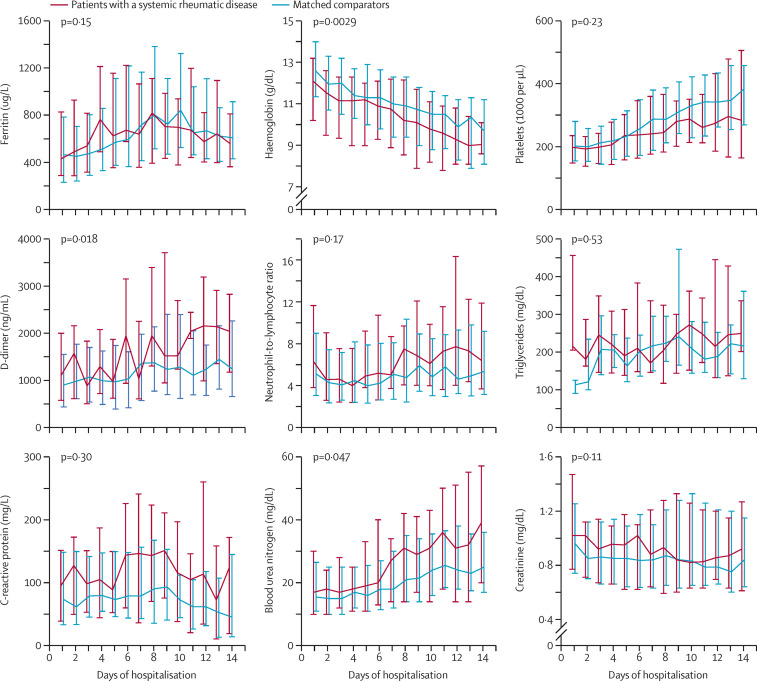
Findings: We identified 57 patients with a systemic rheumatic disease and 232 matched comparators who were admitted to hospital with COVID-19 between Jan 30 and July 7, 2020; 38 (67%) patients with a rheumatic disease were female compared with 158 (68%) matched comparators. Patients with a systemic rheumatic disease had higher peak median neutrophil-to-lymphocyte ratio (9·6 [IQR 6·4-22·2] vs 7·8 [4·5-16·5]; p=0·021), lactate dehydrogenase concentration (421 U/L [297-528] vs 345 U/L [254-479]; p=0·044), creatinine concentration (1·2 mg/dL [0·9-2·0] vs 1·0 mg/dL [0·8-1·4], p=0·014), and blood urea nitrogen concentration (31 mg/dL [15-61] vs 23 mg/dL [13-37]; p=0·033) than comparators, but median C-reactive protein concentration (149·4 mg/L [76·4-275·3] vs 116·3 mg/L [58·8-225·9]; p=0·11) was not significantly different. Patients with a systemic rheumatic disease had higher peak median cHIS than comparators (3 [1-5] vs 2 [1-4]; p=0·013). All patients with a peak cHIS of 2 or more had higher odds of admission to intensive care (OR 3·45 [95% CI 1·98-5·99]), mechanical ventilation (66·20 [8·98-487·80]), and in-hospital mortality (16·37 [4·75-56·38]) than patients with a peak cHIS of less than 2. In adjusted analyses, patients with a rheumatic disease had higher odds of admission to intensive care (2·08 [1·09-3·96]) and mechanical ventilation (2·60 [1·32-5·12]) than comparators, but not in-hospital mortality (1.78 [0·79-4·02]). Among patients who were discharged from hospital, risk of rehospitalisation (1·08 [0·37-3·16]) and mortality within 60 days (1·20 [0·58-2·47]) was similar in patients and comparators.
Interpretation: Patients with a systemic rheumatic disease who were admitted to hospital for COVID-19 had increased risk for hyperinflammation, kidney injury, admission to intensive care, and mechanical ventilation compared with matched comparators. However, among patients who survived, post-discharge outcomes were not significantly different. The cHIS identified patients with hyperinflammation, which was strongly associated with poor COVID-19 outcomes in both patients with a rheumatic disease and comparators. Clinicians should be aware that patients with systemic rheumatic diseases and COVID-19 could be susceptible to hyperinflammation and poor hospital outcomes.
Funding: None.
© 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
HKC has received research support from AstraZeneca and consultancy fees from Takeda, Selecta, GlaxoSmithKline, and Horizon. EMG has an editor position at New England Journal of Medicine and has received royalties from the textbook Rheumatology. ZSW has received research support from Bristol-Myers Squibb and Principia and consulting fees from Viela Bio and MedPace. JAS has received research support from Amgen and Bristol-Myers Squibb and consultancy fees from Bristol-Myers Squibb, Gilead, Inova, Janssen, Optum, and Pfizer. All other authors declare no competing interests.
Figures
Similar articles
-
Clinical criteria for COVID-19-associated hyperinflammatory syndrome: a cohort study.Lancet Rheumatol. 2020 Dec;2(12):e754-e763. doi: 10.1016/S2665-9913(20)30343-X. Epub 2020 Sep 29. Lancet Rheumatol. 2020. PMID: 33015645 Free PMC article.
-
Determinants of COVID-19 disease severity in patients with underlying rheumatic disease.Clin Rheumatol. 2020 Sep;39(9):2789-2796. doi: 10.1007/s10067-020-05301-2. Epub 2020 Jul 27. Clin Rheumatol. 2020. PMID: 32720259 Free PMC article.
-
Assessment of Admission COVID-19 Associated Hyperinflammation Syndrome Score in Critically-Ill COVID-19 Patients.J Intensive Care Med. 2023 Jan;38(1):70-77. doi: 10.1177/08850666221131265. Epub 2022 Oct 10. J Intensive Care Med. 2023. PMID: 36213939 Free PMC article.
-
Coronavirus disease 2019 outcomes among patients with rheumatic diseases 6 months into the pandemic.Ann Rheum Dis. 2021 May;80(5):660-666. doi: 10.1136/annrheumdis-2020-219279. Epub 2020 Nov 30. Ann Rheum Dis. 2021. PMID: 33257496 Free PMC article.
-
Pharmacotherapy in Systemic Rheumatic Diseases.2021 Jan 6. In: Almoallim H, Cheikh M, editors. Skills in Rheumatology [Internet]. Singapore: Springer; 2021. Chapter 4. 2021 Jan 6. In: Almoallim H, Cheikh M, editors. Skills in Rheumatology [Internet]. Singapore: Springer; 2021. Chapter 4. PMID: 36315815 Free Books & Documents. Review.
Cited by
-
Risk factors and outcomes for repeat COVID-19 infection among patients with systemic autoimmune rheumatic diseases: A case-control study.Semin Arthritis Rheum. 2023 Dec;63:152286. doi: 10.1016/j.semarthrit.2023.152286. Epub 2023 Oct 29. Semin Arthritis Rheum. 2023. PMID: 37913612 Free PMC article.
-
Impact of cross-coronavirus immunity in post-acute sequelae of COVID-19.medRxiv [Preprint]. 2022 Sep 26:2022.09.25.22280335. doi: 10.1101/2022.09.25.22280335. medRxiv. 2022. PMID: 36203557 Free PMC article. Preprint.
-
Humoral immunity to an endemic coronavirus is associated with postacute sequelae of COVID-19 in individuals with rheumatic diseases.Sci Transl Med. 2023 Sep 6;15(712):eadf6598. doi: 10.1126/scitranslmed.adf6598. Epub 2023 Sep 6. Sci Transl Med. 2023. PMID: 37672567 Free PMC article.
-
Outcomes with and without outpatient SARS-CoV-2 treatment for patients with COVID-19 and systemic autoimmune rheumatic diseases: a retrospective cohort study.Lancet Rheumatol. 2023 Mar;5(3):e139-e150. doi: 10.1016/S2665-9913(23)00006-1. Epub 2023 Jan 23. Lancet Rheumatol. 2023. PMID: 36844970 Free PMC article.
-
Identifying COVID-19 Confirmed Patients at Elevated Risk for Mortality and Need of Mechanical Ventilation Using a Novel Criteria for Hyperinflammatory Syndrome: A Retrospective Cohort, Single-center, Validation Study.Acta Med Philipp. 2025 Feb 28;59(3):104-115. doi: 10.47895/amp.vi0.9370. eCollection 2025. Acta Med Philipp. 2025. PMID: 40151221 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
