

Cabozantinib and dasatinib synergize to induce tumor regression in non-clear cell renal cell carcinoma
- PMID: 34095877
- PMCID: PMC8149375
- DOI: 10.1016/j.xcrm.2021.100267
Cabozantinib and dasatinib synergize to induce tumor regression in non-clear cell renal cell carcinoma
Abstract
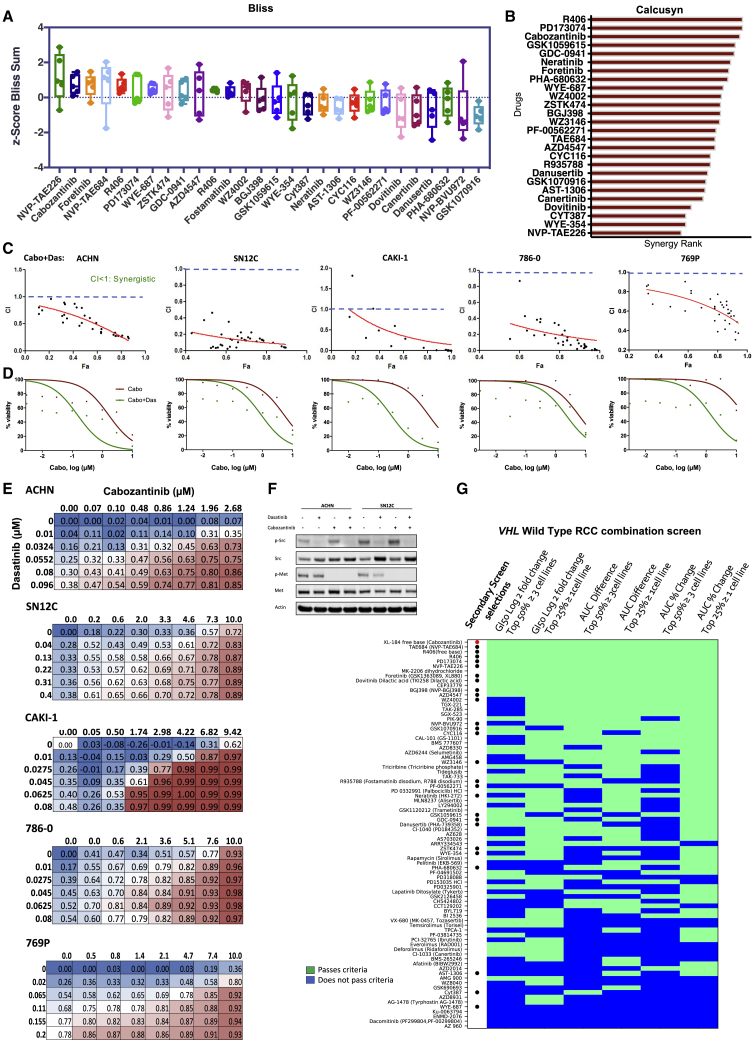
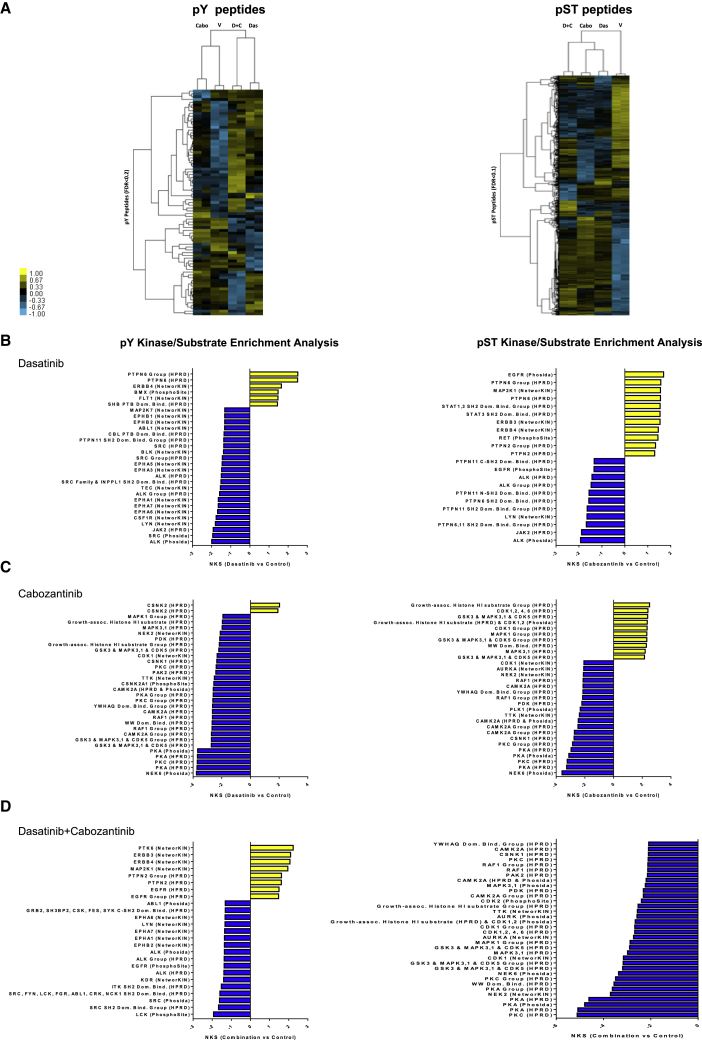
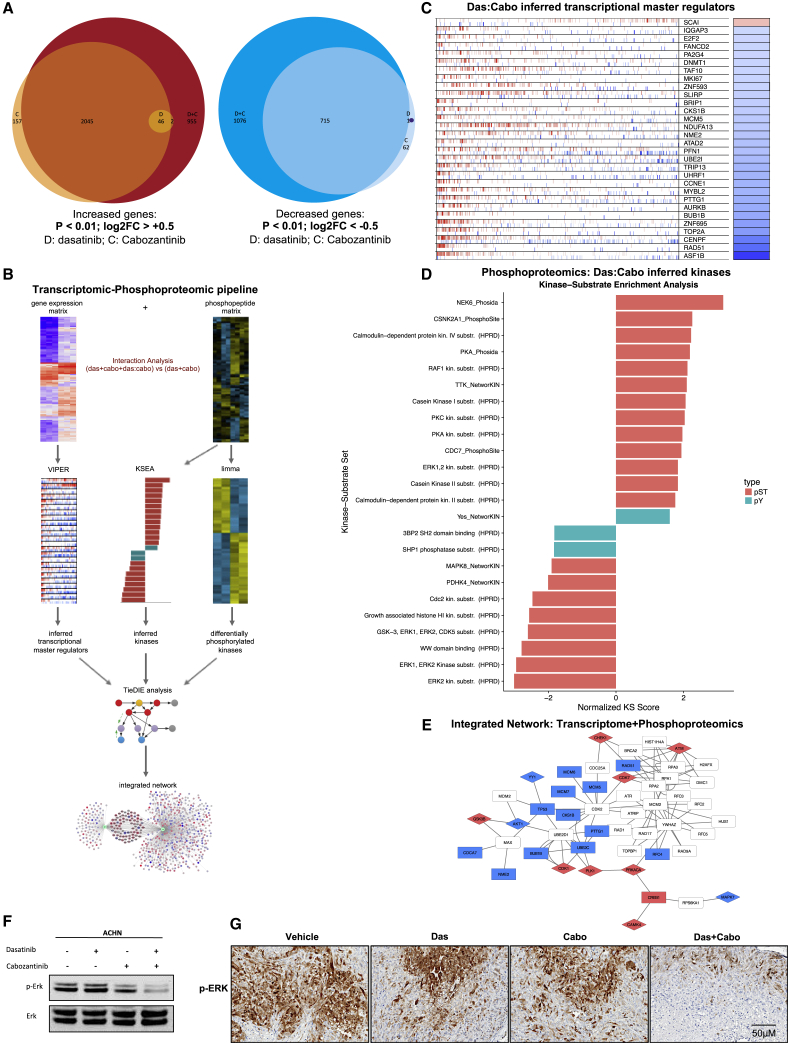
The lack of effective treatment options for advanced non-clear cell renal cell carcinoma (NCCRCC) is a critical unmet clinical need. Applying a high-throughput drug screen to multiple human kidney cancer cells, we identify the combination of the VEGFR-MET inhibitor cabozantinib and the SRC inhibitor dasatinib acts synergistically in cells to markedly reduce cell viability. Importantly, the combination is well tolerated and causes tumor regression in vivo. Transcriptional and phosphoproteomic profiling reveals that the combination converges to downregulate the MAPK-ERK signaling pathway, a result not predicted by single-agent analysis alone. Correspondingly, the addition of a MEK inhibitor synergizes with either dasatinib or cabozantinib to increase its efficacy. This study, by using approved, clinically relevant drugs, provides the rationale for the design of effective combination treatments in NCCRCC that can be rapidly translated to the clinic.
Keywords: MEK; SRC; VEGFR; cabozantinib; cobimetinib; combination therapies; dasatinib; high throughput screen; kidney cancer; non-clear cell renal cell carcinoma.
© 2021 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018;68:394–424. - PubMed
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2018. CA Cancer J. Clin. 2018;68:7–30. - PubMed
-
- George D.J., Kaelin W.G., Jr. The von Hippel-Lindau protein, vascular endothelial growth factor, and kidney cancer. N. Engl. J. Med. 2003;349:419–421. - PubMed
-
- Kaelin W.G., Jr. The von Hippel-Lindau gene, kidney cancer, and oxygen sensing. J. Am. Soc. Nephrol. 2003;14:2703–2711. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
