

Understanding the role of left and right ventricular strain assessment in patients hospitalized with COVID-19
- PMID: 34095889
- PMCID: PMC8168299
- DOI: 10.1016/j.ahjo.2021.100018
Understanding the role of left and right ventricular strain assessment in patients hospitalized with COVID-19
Abstract
Background: Coronavirus disease 2019 (COVID-19) can cause cardiac injury resulting in abnormal right or left ventricular function (RV/LV) with worse outcomes. We hypothesized that two-dimensional (2D) speckle-tracking assessment of LV global longitudinal strain (GLS) and RV free wall strain (FWS) by transthoracic echocardiography can assist as markers for subclinical cardiac injury predicting increased mortality.
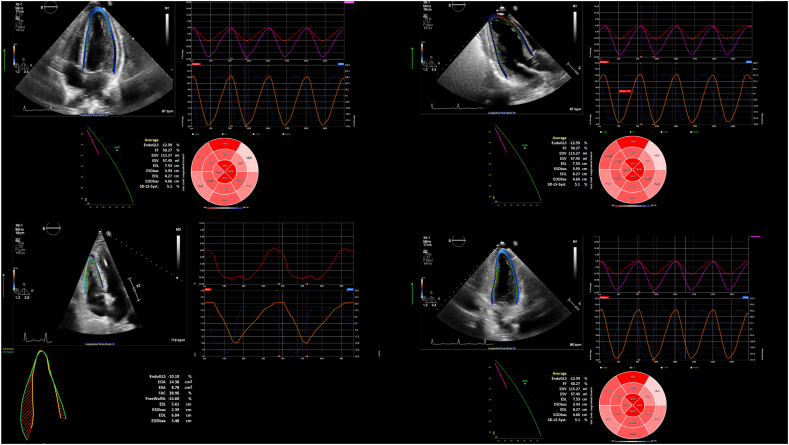
Methods: We performed 2D strain analysis via proprietary software in 48 patients hospitalized with COVID-19. Clinical information, demographics, comorbidities, and lab values were collected via retrospective chart review. The primary outcome was in-hospital mortality based on an optimized abnormal LV GLS value via ROC analysis and RV FWS.
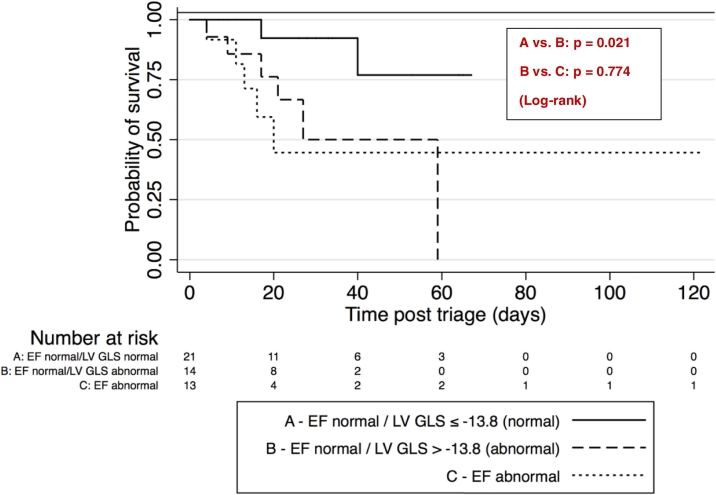
Results: The optimal LV GLS cutoff to predict death was -13.8%, with a sensitivity of 85% (95% CI 55-98%) and specificity of 54% (95% CI 36-71%). Abnormal LV GLS >-13.8% was associated with a higher risk of death [unadjusted hazard ratio 5.15 (95% CI 1.13-23.45), p = 0.034], which persisted after adjustment for clinical variables. Among patients with LV ejection fraction (LVEF) >50%, those with LV GLS > -13.8% had higher mortality compared to those with LV GLS <-13.8% (41% vs. 10%, p = 0.030). RV FWS value was higher in patients with LV GLS >-13.8% (-13.7 ± 5.9 vs. -19.6 ± 6.7, p = 0.003), but not associated with decreased survival.
Conclusion: Abnormal LV strain with a cutoff of >-13.8% in patients with COVID-19 is associated with significantly higher risk of death. Despite normal LVEF, abnormal LV GLS predicted worse outcomes in patients hospitalized with COVID-19. There was no mortality difference based on RV strain.
Keywords: 2D, Two-dimensional; ARDS, acute respiratory distress syndrome; COVID-19; COVID-19, Coronavirus Disease 2019; EF, ejection fraction; FAC, fractional area change; FWS, free wall strain; GLS, global longitudinal strain; HFrEF, heart failure reduced ejection fraction; Hs-TNT, high sensitivity troponin T; ICC, intra-class correlation coefficient; LV, left ventricle; Left ventricular strain; NT-proBNP, NT-pro-brain natriuretic peptide; RV, right ventricle; Speckle-tracking echocardiography; TTE, transthoracic echocardiography.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Mizuguchi Y., Oishi Y., Miyoshi H., Iuchi A., Nagase N., Oki T. The functional role of longitudinal, circumferential, and radial myocardial deformation for regulating the early impairment of left ventricular contraction and relaxation in patients with cardiovascular risk factors: a study with two-dimensional strain Im. J. Am. Soc. Echocardiogr. 2008 doi: 10.1016/j.echo.2008.07.016. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
