

COVID-19 pandemic and population-level pregnancy and neonatal outcomes: a living systematic review and meta-analysis
- PMID: 34096034
- PMCID: PMC8222877
- DOI: 10.1111/aogs.14206
COVID-19 pandemic and population-level pregnancy and neonatal outcomes: a living systematic review and meta-analysis
Abstract
Introduction: Conflicting reports of increases and decreases in rates of preterm birth (PTB) and stillbirth in the general population during the COVID-19 pandemic have surfaced. The objective of our study was to conduct a living systematic review and meta-analyses of studies reporting pregnancy and neonatal outcomes by comparing the pandemic and pre-pandemic periods.
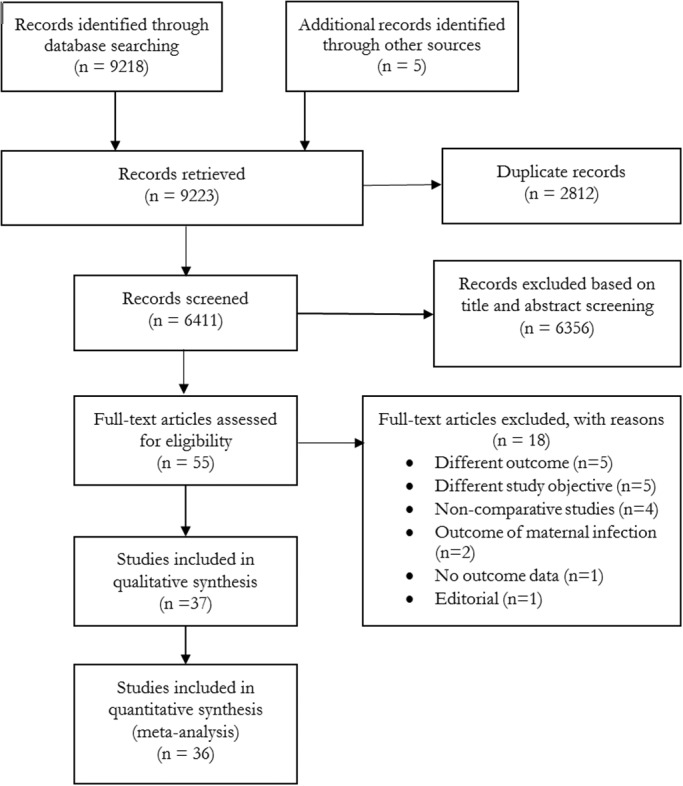
Material and methods: We searched PubMed and Embase databases, reference lists of articles published up until 14 May 2021 and included English language studies that compared outcomes between the COVID-19 pandemic time period and pre-pandemic time periods. Risk of bias was assessed using the Newcastle-Ottawa scale. We conducted random-effects meta-analysis using the inverse variance method.
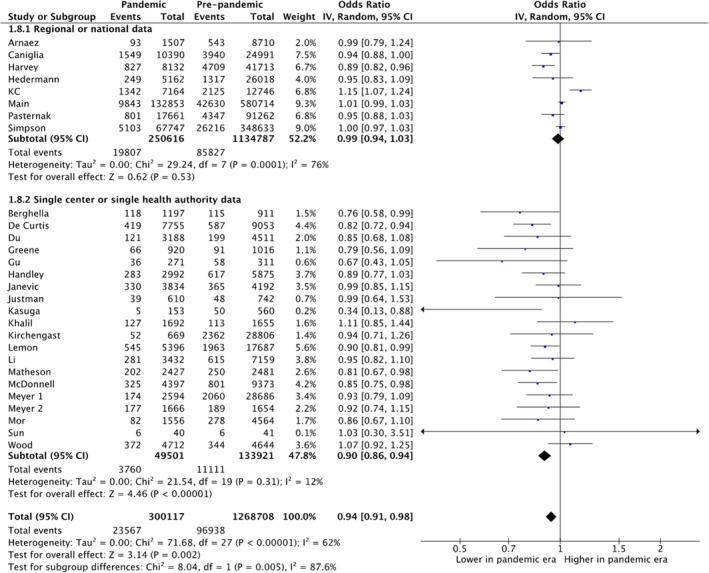
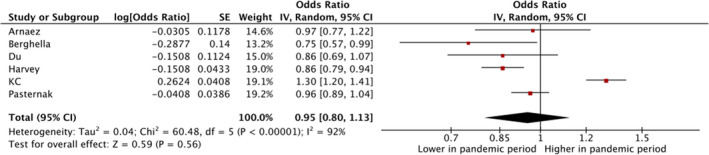
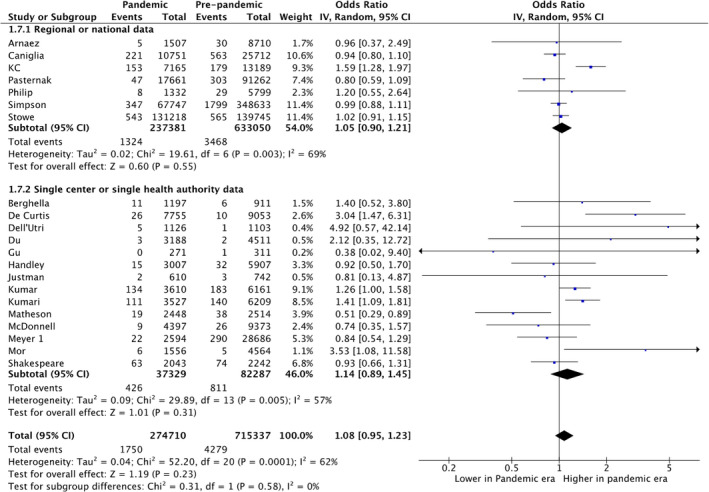
Results: Thirty-seven studies with low-to-moderate risk of bias, reporting on 1 677 858 pregnancies during the pandemic period and 21 028 650 pregnancies during the pre-pandemic period, were included. There was a significant reduction in unadjusted estimates of PTB (28 studies, unadjusted odds ratio [uaOR] 0.94, 95% confidence [CI] 0.91-0.98) but not in adjusted estimates (six studies, adjusted OR [aOR] 0.95, 95% CI 0.80-1.13). The reduction was noted in studies from single centers/health areas (uaOR 0.90, 95% CI 0.86-0.94) but not in regional/national studies (uaOR 0.99, 95% CI 0.95-1.03). There was reduction in spontaneous PTB (five studies, uaOR 0.89, 95% CI 0.82-0.98) and induced PTB (four studies, uaOR 0.90, 95% CI 0.81-1.00). There was no reduction in PTB when stratified by gestational age <34, <32 or <28 weeks. There was no difference in stillbirths between the pandemic and pre-pandemic time periods (21 studies, uaOR 1.08, 95% CI 0.94-1.23; four studies, aOR 1.06, 95% CI 0.81-1.38). There was an increase in birthweight (six studies, mean difference 17 g, 95% CI 7-28 g) during the pandemic period. There was an increase in maternal mortality (four studies, uaOR 1.15, 95% CI 1.05-1.26), which was mostly influenced by one study from Mexico. There was significant publication bias for the outcome of PTB.
Conclusions: The COVID-19 pandemic time period may be associated with a reduction in PTB; however, referral bias cannot be excluded. There was no difference in stillbirth between the pandemic and pre-pandemic period.
Keywords: SARS-CoV-2; birthweight; epidemic; maternal mortality; neonatal mortality; preterm birth; stillbirth; stress.
© 2021 Nordic Federation of Societies of Obstetrics and Gynecology.
Conflict of interest statement
None.
Figures

References
-
- Ohlsson A, Shah PS. Effects of the September 11, 2001 disaster on pregnancy outcomes: a systematic review. Acta Obstet Gynecol Scand. 2011;90:6‐18. - PubMed
-
- Philip RK, Purtill H, Reidy E, et al. Unprecedented reduction in births of very low birthweight (VLBW) and extremely low birthweight (ELBW) infants during the COVID‐19 lockdown in Ireland: a ‘natural experiment’ allowing analysis of data from the prior two decades. BMJ Glob Health. 2020;5:e003075. - PMC - PubMed
-
- Liu LI, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post‐2015 priorities: an updated systematic analysis. Lancet. 2015;385:430‐440. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
