

Evaluation of Emergency Department Pediatric Readiness and Outcomes Among US Trauma Centers
- PMID: 34096991
- PMCID: PMC8185631
- DOI: 10.1001/jamapediatrics.2021.1319
Evaluation of Emergency Department Pediatric Readiness and Outcomes Among US Trauma Centers
Abstract
Importance: The National Pediatric Readiness Project is a US initiative to improve emergency department (ED) readiness to care for acutely ill and injured children. However, it is unclear whether high ED pediatric readiness is associated with improved survival in US trauma centers.
Objective: To evaluate the association between ED pediatric readiness, in-hospital mortality, and in-hospital complications among injured children presenting to US trauma centers.
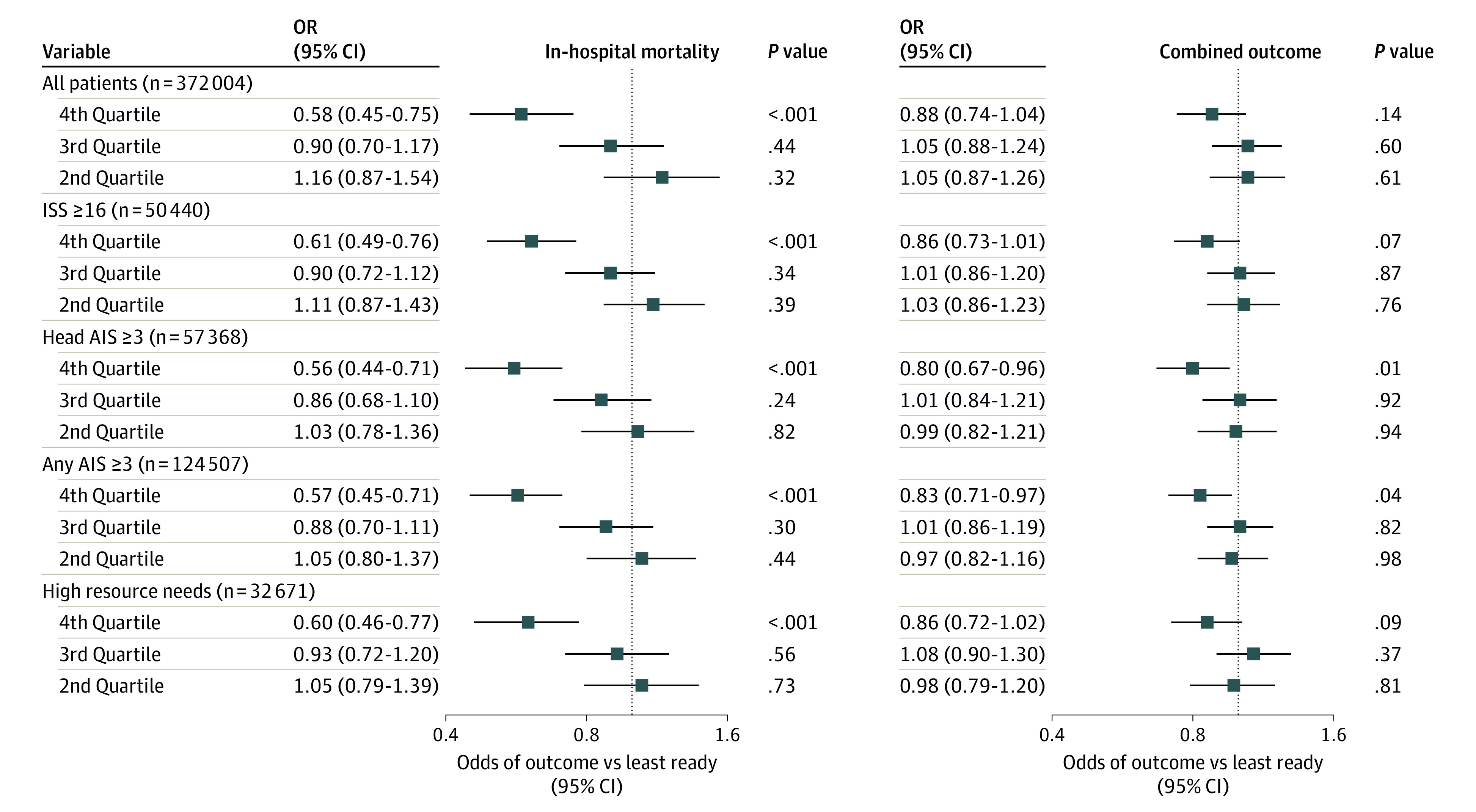
Design, setting, and participants: A retrospective cohort study of 832 EDs in US trauma centers in 50 states and the District of Columbia was conducted using data from January 1, 2012, through December 31, 2017. Injured children younger than 18 years who were admitted, transferred, or with injury-related death in a participating trauma center were included in the analysis. Subgroups included children with an Injury Severity Score (ISS) of 16 or above, indicating overall seriously injured (accounting for all injuries); any Abbreviated Injury Scale (AIS) score of 3 or above, indicating at least 1 serious injury; a head AIS score of 3 or above, indicating serious brain injury; and need for early use of critical resources.
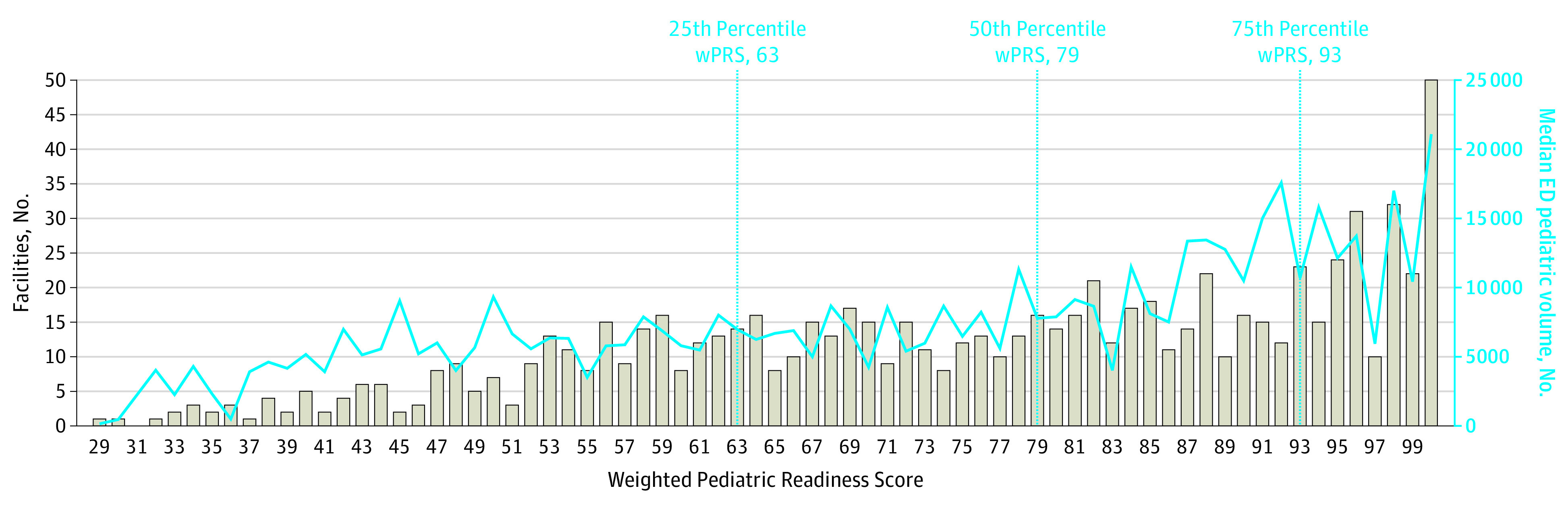
Exposures: Emergency department pediatric readiness for the initial ED visit, measured through the weighted Pediatric Readiness Score (range, 0-100) from the 2013 National Pediatric Readiness Project ED pediatric readiness assessment.
Main outcomes and measures: In-hospital mortality, with a secondary composite outcome of in-hospital mortality or complication. For the primary measurement tools used, the possible range of the AIS is 0 to 6, with 3 or higher indicating a serious injury; the possible range of the ISS is 0 to 75, with 16 or higher indicating serious overall injury. The weighted Pediatric Readiness Score examines and scores 6 domains; in this study, the lowest quartile included scores of 29 to 62 and the highest quartile included scores of 93 to 100.
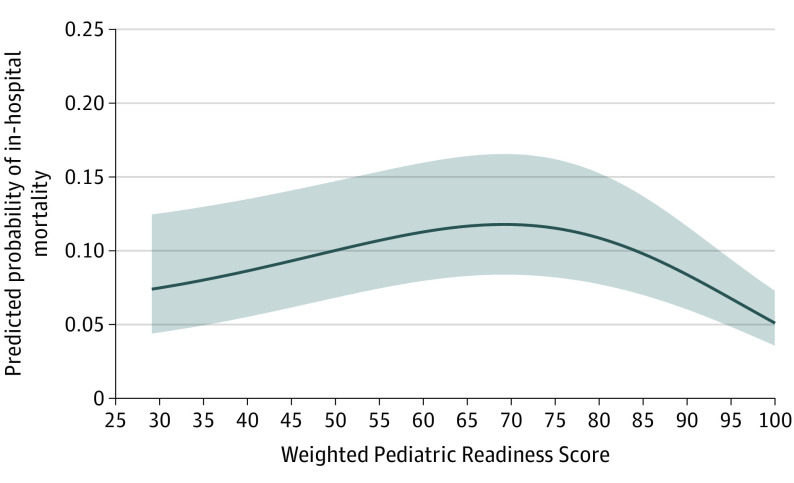
Results: There were 372 004 injured children (239 273 [64.3%] boys; median age, 10 years [interquartile range, 4-15 years]), including 5700 (1.5%) who died in-hospital and 5018 (1.3%) who developed in-hospital complications. Subgroups included 50 440 children (13.6%) with an ISS of 16 or higher, 124 507 (33.5%) with any AIS score of 3 or higher, 57 368 (15.4%) with a head AIS score of 3 or higher, and 32 671 (8.8%) requiring early use of critical resources. Compared with EDs in the lowest weighted Pediatric Readiness Score quartile, children cared for in the highest ED quartile had lower in-hospital mortality (adjusted odds ratio [aOR], 0.58; 95% CI, 0.45-0.75), but not fewer complications (aOR for the composite outcome 0.88; 95% CI, 0.74-1.04). These findings were consistent across subgroups, strata, and multiple sensitivity analyses. If all children cared for in the lowest-readiness quartiles (1-3) were treated in an ED in the highest quartile of readiness, an additional 126 lives (95% CI, 97-154 lives) might be saved each year in these trauma centers.
Conclusions and relevance: In this cohort study, injured children treated in high-readiness EDs had lower mortality compared with similar children in low-readiness EDs, but not fewer complications. These findings support national efforts to increase ED pediatric readiness in US trauma centers that care for children.
Conflict of interest statement
Figures
References
-
- National Center for Injury Prevention and Control CNVSS, National Center for Health Statistics . 10 Leading causes of death by age group, United States—2012. National Center for Injury Prevention and Control CNVSS, National Center for Health Statistics; 2014.
-
- Borse NNRR, Dellinger AM, Sleet DA; Centers for Disease Control and Prevention (CDC) . Years of potential life lost from unintentional injuries among persons aged 0-19 years—United States, 2000-2009. MMWR Morb Mortal Wkly Rep. 2012;61(41):830-833. - PubMed
-
- McDermott KW, Stocks C, Freeman WJ. Overview of Pediatric Emergency Department Visits, 2015. HCUP Statistical Brief #242. Agency for Healthcare Research and Quality; August 2018. - PubMed
-
- Institute of Medicine, Committee on the Future of Emergency Care in the United States Health System . Emergency Care for Children: Growing Pains. National Academy Press; 2006. - PubMed
-
- The National Pediatric Readiness Project , Emergency Medical Services for Children (EMSC) National Resource Center. Accessed February 19, 2021. http://www.pediatricreadiness.org/
