

Racial, Ethnic, and Gender Representation in Leadership Positions at National Cancer Institute-Designated Cancer Centers
- PMID: 34097046
- PMCID: PMC8185594
- DOI: 10.1001/jamanetworkopen.2021.12807
Racial, Ethnic, and Gender Representation in Leadership Positions at National Cancer Institute-Designated Cancer Centers
Abstract
Importance: Increasing diversity is beneficial for the health care system and patient outcomes; however, the current leadership gap in oncology remains largely unquantified.
Objective: To evaluate the gender, racial, and ethnic makeup of the leadership teams of National Cancer Institute (NCI)-designated cancer centers and compare with the city populations served by each center.
Design, setting, and participants: This retrospective cross-sectional study examined gender, race, and ethnicity of leadership teams via publicly available information for NCI-designated cancer centers and compared results with national and city US census population characteristics, as well as active physician data. Data were analyzed in August 2020.
Main outcomes and measures: Racial, ethnic, and gender diversity (identified via facial recognition software and manual review) of leadership teams compared with institution rank, location, team member degree(s), and h-index.
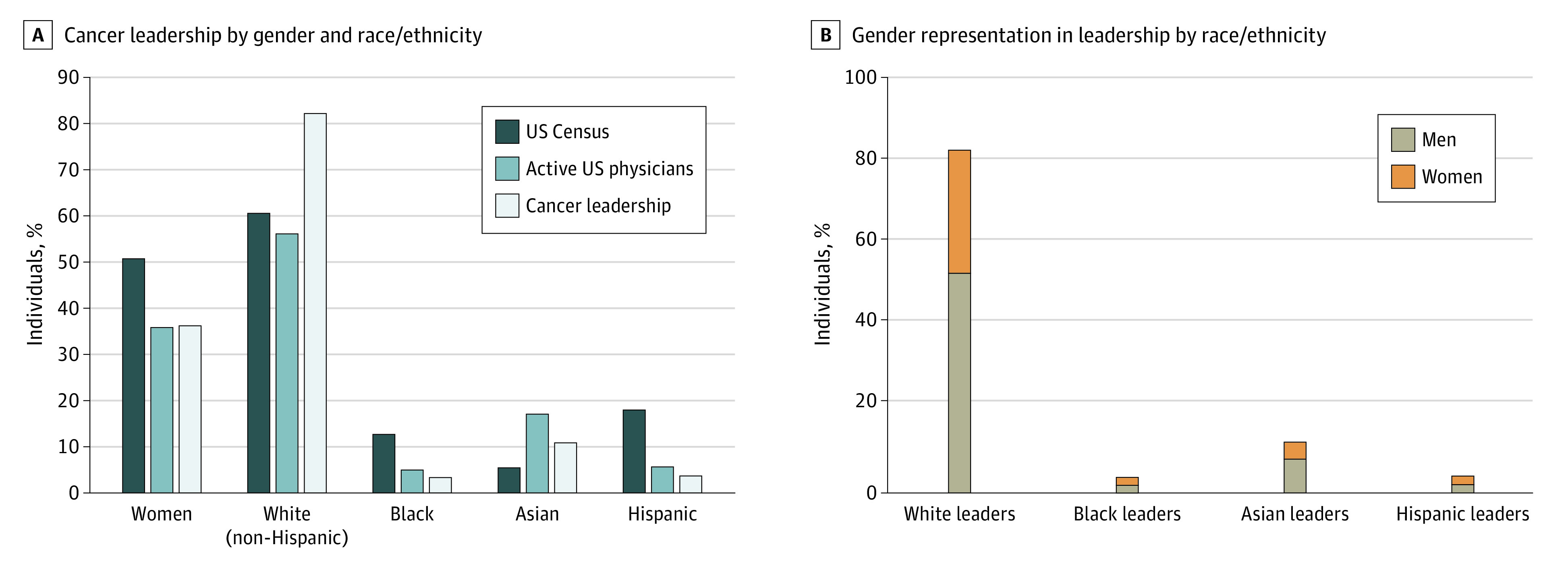
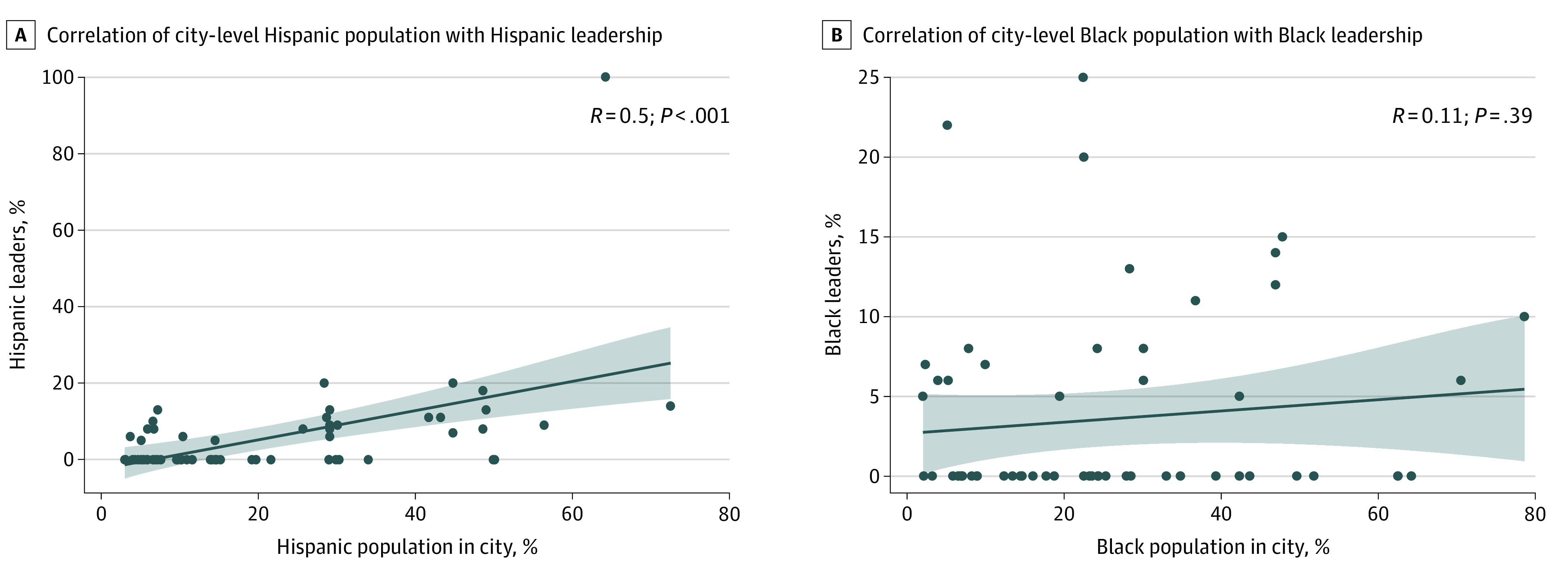
Results: All 63 NCI cancer centers were included in analysis, and all had identifiable leadership teams, with a total of 856 members. Photographs were not identified for 12 leaders (1.4%); of the remaining 844 leaders, race/ethnicity could not be identified for 7 (0.8%). Women make up 50.8% of the US population and 35.9% of active physicians; in NCI cancer centers, 36.3% (306 women) of cancer center leaders were women. Non-Hispanic White individuals comprise 60.6% of the US population and 56.2% of active physicians, but 82.2% of cancer center leaders (688 individuals) were non-Hispanic White. Both Black and Hispanic physicians were underrepresented when compared with their census populations (Black: 12.7% of US population, 5.0% of active physicians; Hispanic: 18.1% of US population, 5.8% of active physicians); however, Black and Hispanic individuals were even less represented in cancer center leadership positions (29 Black leaders [3.5%]; 32 Hispanic leaders [3.8%]). Asian physicians were overrepresented compared with their census population (5.6% of US population, 17.1% of active physicians); however, Asian individuals were underrepresented in leadership positions (92 Asian individuals [11.0%]). A total of 23 NCI cancer centers (36.5%) did not have a single Black or Hispanic member of their leadership team; 8 cancer centers (12.7%) had an all non-Hispanic White leadership team. A multivariate model found that leadership teams with more women (adjusted odds ratio, 1.73 [95% CI, 1.02-2.93]; P = .04) and institutions in the South (adjusted odds ratio, 2.31 [95% CI, 1.15 to 4.77]; P = .02) were more likely to have at least 1 Black or Hispanic leader. Pearson correlation analysis showed weak to moderate correlation between city Hispanic population and Hispanic representation on leadership teams (R = 0.5; P < .001), but no significant association between Black population and Black leadership was found.
Conclusions and relevance: This cross-sectional study found that significant racial and ethnic disparities were present in cancer center leadership positions. Establishing policy, as well as pipeline programs, to address these disparities is essential for change.
Conflict of interest statement
Figures
References
-
- Zeng C, Wen W, Morgans AK, Pao W, Shu XO, Zheng W. Disparities by race, age, and sex in the improvement of survival for major cancers: results from the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program in the United States, 1990 to 2010. JAMA Oncol. 2015;1(1):88-96. doi: 10.1001/jamaoncol.2014.161 - DOI - PMC - PubMed
-
- McKinsey & Company . Delivering through diversity. Accessed November 12, 2020. https://www.mckinsey.com/~/media/mckinsey/business%20functions/organizat...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
