

Protective ventilation and outcomes of critically ill patients with COVID-19: a cohort study
- PMID: 34097145
- PMCID: PMC8182738
- DOI: 10.1186/s13613-021-00882-w
Protective ventilation and outcomes of critically ill patients with COVID-19: a cohort study
Abstract
Background: Approximately 5% of COVID-19 patients develop respiratory failure and need ventilatory support, yet little is known about the impact of mechanical ventilation strategy in COVID-19. Our objective was to describe baseline characteristics, ventilatory parameters, and outcomes of critically ill patients in the largest referral center for COVID-19 in Sao Paulo, Brazil, during the first surge of the pandemic.
Methods: This cohort included COVID-19 patients admitted to the intensive care units (ICUs) of an academic hospital with 94 ICU beds, a number expanded to 300 during the pandemic as part of a state preparedness plan. Data included demographics, advanced life support therapies, and ventilator parameters. The main outcome was 28-day survival. We used a multivariate Cox model to test the association between protective ventilation and survival, adjusting for PF ratio, pH, compliance, and PEEP.
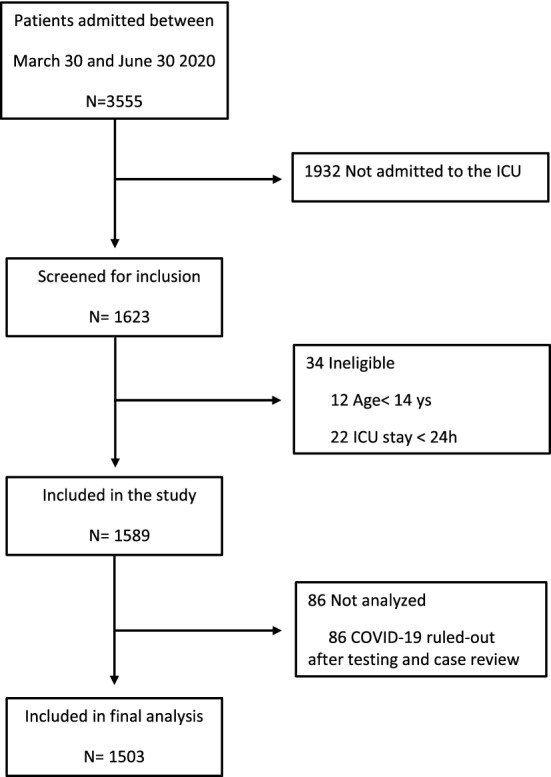
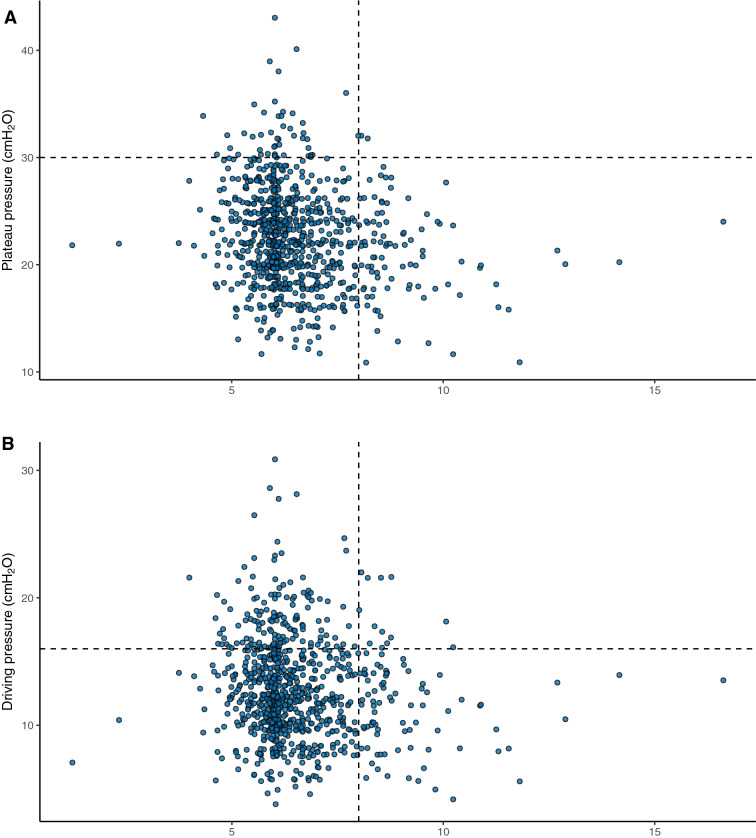
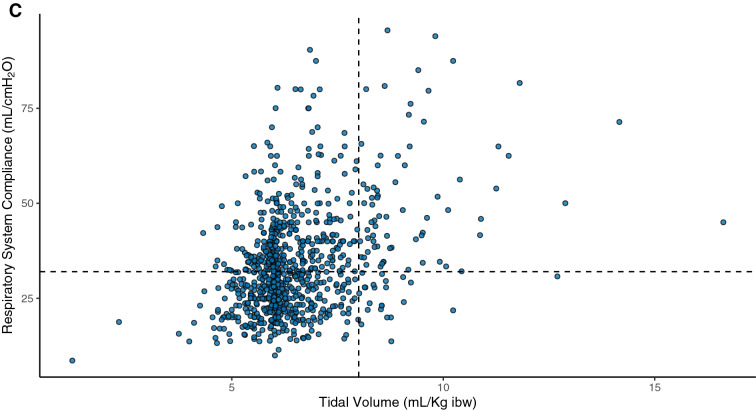
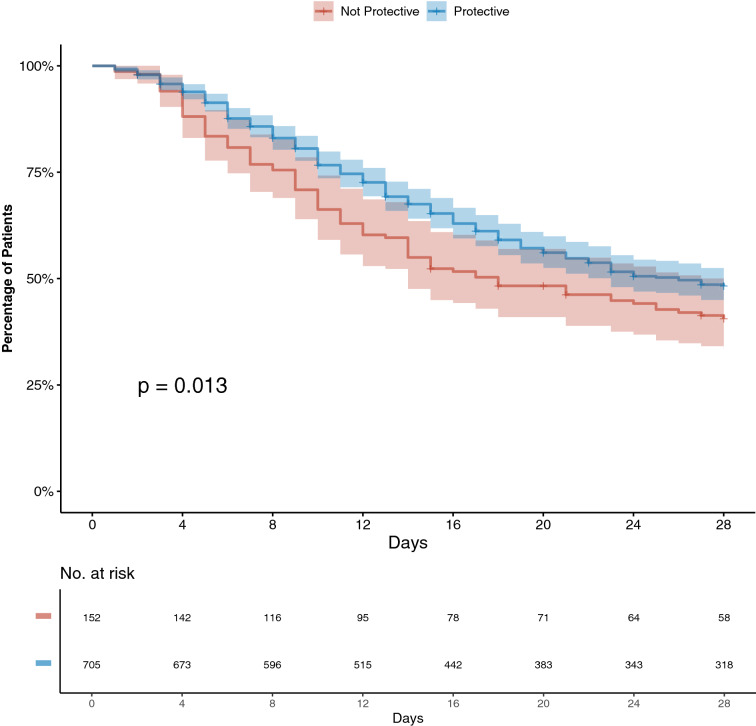
Results: We included 1503 patients from March 30 to June 30, 2020. The mean age was 60 ± 15 years, and 59% were male. During 28-day follow-up, 1180 (79%) patients needed invasive ventilation and 666 (44%) died. For the 984 patients who were receiving mechanical ventilation in the first 24 h of ICU stay, mean tidal volume was 6.5 ± 1.3 mL/kg of ideal body weight, plateau pressure was 24 ± 5 cmH2O, respiratory system compliance was 31.9 (24.4-40.9) mL/cmH2O, and 82% of patients were ventilated with protective ventilation. Noninvasive ventilation was used in 21% of patients, and prone, in 36%. Compliance was associated with survival and did not show a bimodal pattern that would support the presence of two phenotypes. In the multivariable model, protective ventilation (aHR 0.73 [95%CI 0.57-0.94]), adjusted for PF ratio, compliance, PEEP, and arterial pH, was independently associated with survival.
Conclusions: During the peak of the epidemic in Sao Paulo, critically ill patients with COVID-19 often required mechanical ventilation and mortality was high. Our findings revealed an association between mechanical ventilation strategy and mortality, highlighting the importance of protective ventilation for patients with COVID-19.
Keywords: COVID-19; Pneumonia, viral; SARS virus; Severe acute respiratory syndrome; Ventilation, artificial.
Conflict of interest statement
Dr. Ferreira reports personal fees from Medtronic, outside the submitted work; Dr. Ho reports personal fees from Pan-American Health Organization, outside the submitted work; Dr. Besen reports personal fees from Cristália, outside the submitted work. Dr. Costa reports personal fees from Timpel, personal fees from Magnamed, outside the submitted work. The other authors have no conflict of interest to disclose.
Figures
References
-
- Johns Hopkins University. COVID-19 Map - Johns Hopkins Coronavirus Resource Center https://coronavirus.jhu.edu/map.html. Accessed 8 Febr 2021.
-
- Seade, Governo de São Paulo, Coronavírus dados Completos, Brasil. https://www.seade.gov.br/coronavirus/. Accessed 8 Febr 2021.
LinkOut - more resources
Full Text Sources
Miscellaneous
