

Associations between measures of pediatric human resources and the under-five mortality rate: a nationwide study in China in 2014
- PMID: 34097241
- PMCID: PMC8183000
- DOI: 10.1007/s12519-021-00433-0
Associations between measures of pediatric human resources and the under-five mortality rate: a nationwide study in China in 2014
Abstract
Background: To quantify the associations between the under-five mortality rate (U5MR) and measures of pediatric human resources, including pediatricians per thousand children (PPTC) and the geographical distribution of pediatricians.
Methods: We analyzed data from a national survey in 2015-2016 in 2636 counties, accounting for 31 mainland provinces of China. We evaluated the associations between measures of pediatric human resources and the risk of a high U5MR (≥ 18 deaths per 1000 live births) using logistic regression and restricted cubic spline regression models with adjustments for potential confounders. PPTC and pediatricians per 10,000 km2 were categorized into quartiles. The highest quartiles were used as reference.
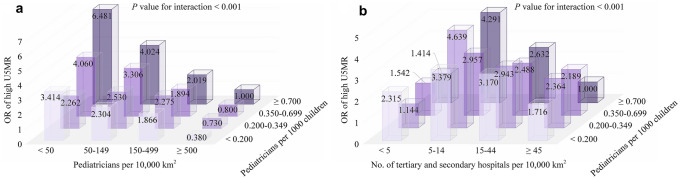
Results: The median values of PPTC and pediatricians per 10,000 km2 were 0.35 (0.20-0.70) and 150 (50-500), respectively. Compared to the counties with the highest PPTC (≥ 0.7), those with the lowest PPTC (< 0.2) had a 52% higher risk of a high U5MR, with an L-shaped relationship. An inverted J-shaped relationship was found that the risk of a high U5MR was 3.74 [95% confidence interval (CI) 2.55-5.48], 3.07 (95% CI 2.11-4.47), and 2.25 times (95% CI 1.52-3.31) higher in counties with < 50, 50-149, and 150-499 pediatricians per 10,000 km2, respectively, than in counties with ≥ 500 physicians per 10,000 km2. The joint association analyses show a stronger association with the risk of a high U5MR in geographical pediatrician density than PPTC.
Conclusion: Both population and geographical pediatrician density should be considered when planning child health care services, even in areas with high numbers of PPTC.
Keywords: China; Human resources for health; Inequality; National survey; Pediatrician.
Conflict of interest statement
The authors declared that there is no conflict of interest.
Figures

Similar articles
-
Child mortality patterns in rural areas of Anhui and Henan provinces in China, 1990.Biomed Environ Sci. 1998 Sep;11(3):264-76. Biomed Environ Sci. 1998. PMID: 9861486
-
Can a Multi-Component Intervention Improve Pediatric Service Delivery in Guangzhou?Front Public Health. 2021 Oct 4;9:760124. doi: 10.3389/fpubh.2021.760124. eCollection 2021. Front Public Health. 2021. PMID: 34671589 Free PMC article.
-
The impact of the health care workforce on under-five mortality in rural China.Hum Resour Health. 2019 Mar 18;17(1):21. doi: 10.1186/s12960-019-0357-5. Hum Resour Health. 2019. PMID: 30885196 Free PMC article.
-
Greenness on mortality of infant and under-5 child: A nationwide study in 147 Chinese cities.Ecotoxicol Environ Saf. 2024 Nov 1;286:117184. doi: 10.1016/j.ecoenv.2024.117184. Epub 2024 Oct 19. Ecotoxicol Environ Saf. 2024. PMID: 39427541
-
Trends, influencing factors and prediction analysis of under-five and maternal mortality rates in China from 1991 to 2020.Front Public Health. 2023 Oct 19;11:1198356. doi: 10.3389/fpubh.2023.1198356. eCollection 2023. Front Public Health. 2023. PMID: 37927855 Free PMC article.
Cited by
-
Attitudes and perspectives of 534 Chinese pediatricians toward internet hospitals.Front Pediatr. 2022 Sep 28;10:948788. doi: 10.3389/fped.2022.948788. eCollection 2022. Front Pediatr. 2022. PMID: 36245742 Free PMC article.
-
Burden of cardiovascular disease among the Western Pacific region and its association with human resources for health, 1990-2021: a systematic analysis of the Global Burden of Disease Study 2021.Lancet Reg Health West Pac. 2024 Sep 3;51:101195. doi: 10.1016/j.lanwpc.2024.101195. eCollection 2024 Oct. Lancet Reg Health West Pac. 2024. PMID: 39286450 Free PMC article.
-
Spatiotemporal dynamics and driving factors of human resources for health in traditional Chinese medicine in China.Sci Rep. 2025 May 25;15(1):18224. doi: 10.1038/s41598-025-02615-6. Sci Rep. 2025. PMID: 40415058 Free PMC article.
References
-
- The World Bank. World development indicators. Washington DC: The World Bank; 2010–2012.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
