

Comparative study of AQP4-NMOSD, MOGAD and seronegative NMOSD: a single-center Belgian cohort
- PMID: 34097296
- PMCID: PMC8894224
- DOI: 10.1007/s13760-021-01712-3
Comparative study of AQP4-NMOSD, MOGAD and seronegative NMOSD: a single-center Belgian cohort
Abstract
Purpose: To emphasize physio-pathological, clinical and prognosis differences between conditions causing serious and sometimes very similar clinical manifestations: anti-aquaporin-4 (AQP4) and anti-myelin oligodendrocyte glycoprotein (MOG) antibodies related diseases, and seronegative NMOSD (neuromyelitis optica spectrum disorders).
Methods: Based on Wingerchuk et al. (Neurology 85:177-189, 2015) criteria for NMOSD and on those more recently proposed by Jarius et al. (J Neuroinflammation 15:134, 2018) for MOGAD (MOG associated disorders), we retrospectively surveyed 10 AQP4-NMOSD, 8 MOGAD and 2 seronegative NMOSD, followed at the specialized neuroimmunology unit of the CHU Liège.
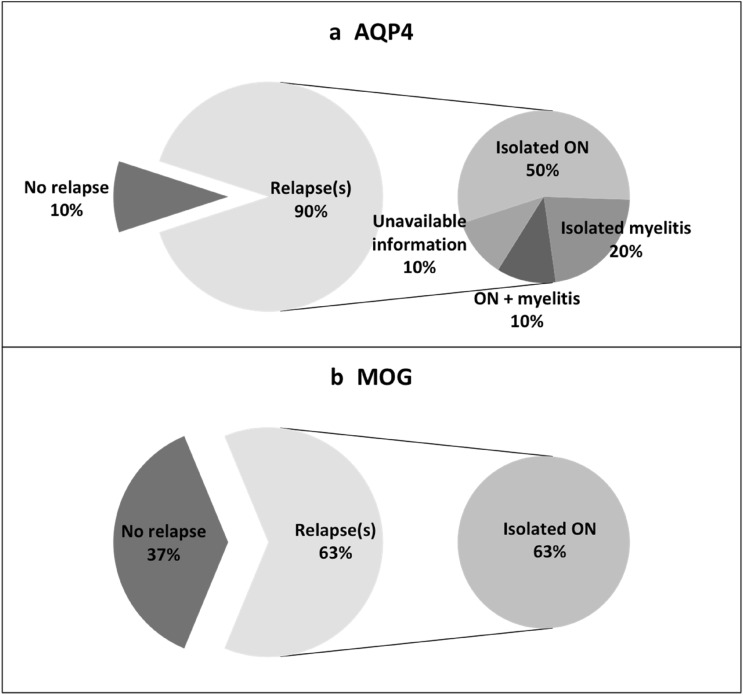
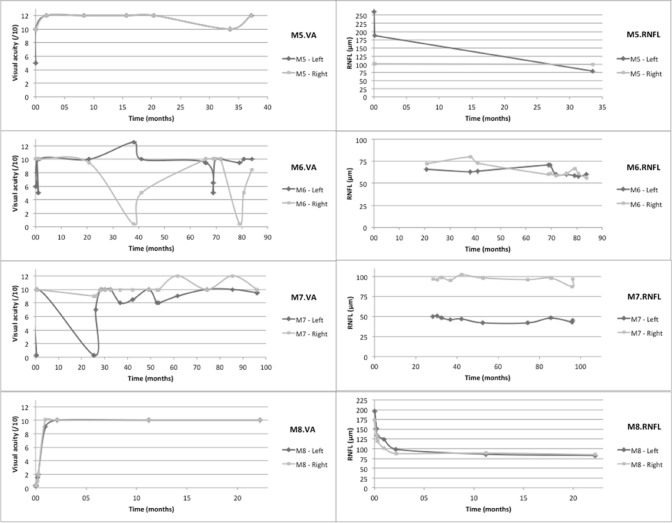
Results: Female predominance was only observed in AQP4 group. Age at onset was 37.8 and 27.7 years old for AQP4-NMOSD and MOGAD respectively. In both groups, the first clinical event most often consisted of optic neuritis (ON), followed by isolated myelitis. Fifteen of our 20 patients encountered a relapsing course with 90% relapses in AQP4-NMOSD, 62.5% in MOGAD and 50% in seronegative group, and a mean period between first and second clinical event of 7.1 and 4.8 months for AQP4-NMOSD and MOGAD, respectively. In total we counted 54 ON, with more ON per patient in MOGAD. MOG-associated ON mainly affected the anterior part of the optic nerve with a papilledema in 79.2% of cases. Despite a fairly good visual outcome after MOG-associated ON, retinal nerve fibre layer (RNFL) thickness decreased, suggesting a fragility of the optic nerve toward further attacks.
Conclusion: As observed in larger cohorts, our MOGAD and AQP4-NMOSD cases differ by clinical and prognostic features. A better understanding of these diseases should encourage prompt biological screening and hasten proper diagnosis and treatment.
Keywords: AQP4-antibody NMO spectrum disorders; MOG-associated disorders; Neuromyelitis optica; Optic neuritis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Devic E. Myélite subaigüe compliquée de névrite optique. Bull Med. 1894;8:1033–1034.
-
- Gault F (1894) De la neuromyélite optique aiguë. Lyon
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
