

Clinical outcomes of modifying hypertension treatment intensity in older adults treated to low blood pressure
- PMID: 34097300
- PMCID: PMC8497391
- DOI: 10.1111/jgs.17295
Clinical outcomes of modifying hypertension treatment intensity in older adults treated to low blood pressure
Abstract
Background/objectives: Hypertension treatment reduces cardiovascular events. However, uncertainty remains about benefits and harms of deintensification or further intensification of antihypertensive medication when systolic blood pressure (SBP) is tightly controlled in older multimorbid patients, because of their frequent exclusion in trials. We assessed the association of hypertension treatment deintensification or intensification with clinical outcomes in older adults with tightly controlled SBP.
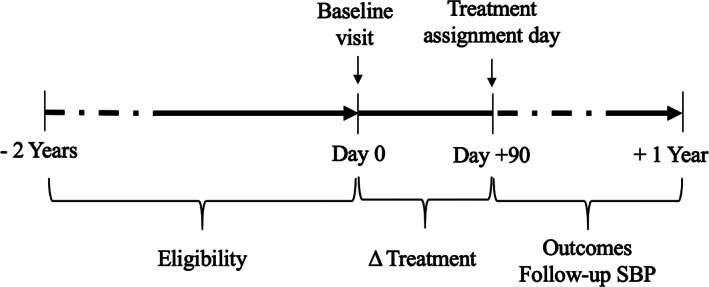
Design: Longitudinal cohort study (2011-2013) with 9-month follow-up.
Setting: U.S.-nationwide primary care Veterans Health Administration healthcare system.
Participants: Veterans aged 65 and older with baseline SBP <130 mmHg and ≥1 antihypertensive medication during ≥2 consecutive visits (N = 228,753).
Exposure: Deintensification or intensification, compared with stable treatment.
Main outcomes and measures: Cardiovascular events, syncope, or fall injury, as composite and distinct outcomes, within 9 months after exposure. Adjusted logistic regression and inverse probability of treatment weighting (IPTW, sensitivity analysis).
Results: Among 228,753 patients (mean age 75 [SD 7.5] years), the composite outcome occurred in 11,982/93,793 (12.8%) patients with stable treatment, 14,768/72,672 (20.3%) with deintensification, and 11,821/62,288 (19.0%) with intensification. Adjusted absolute outcome risk (95% confidence interval) was higher for deintensification (18.3% [18.1%-18.6%]) and intensification (18.7% [18.4%-19.0%]), compared with stable treatment (14.8% [14.6%-15.0%]), p < 0.001 for both effects in the multivariable model). Deintensification was associated with fewer cardiovascular events than intensification. At baseline SBP <95 mmHg, cardiovascular event risk was similar for deintensification and stable treatment, and fall risk lower for deintensification than intensification. IPTW yielded similar results. Mean follow-up SBP was 124.1 mmHg for stable treatment, 125.1 mmHg after deintensification (p < 0.001), and 124.0 mmHg after intensification (p < 0.001).
Conclusion: Antihypertensive treatment deintensification in older patients with tightly controlled SBP was associated with worse outcomes than continuing same treatment intensity. Given higher mortality among patients with treatment modification, confounding by indication may not have been fully corrected by advanced statistical methods for observational data analysis.
Keywords: Veterans; cardiovascular event; deintensification; elderly; fall injury; hypertension; intensification; syncope; treatment.
© 2021 The Authors. Journal of the American Geriatrics Society published by Wiley Periodicals LLC on behalf of The American Geriatrics Society.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures

Similar articles
-
Factors associated with antihypertensive treatment intensification and deintensification in older outpatients.Int J Cardiol Hypertens. 2021 Jun 23;9:100098. doi: 10.1016/j.ijchy.2021.100098. eCollection 2021 Jun. Int J Cardiol Hypertens. 2021. PMID: 34258575 Free PMC article.
-
Effects of blood pressure-lowering treatment on cardiovascular outcomes and mortality: 13 - benefits and adverse events in older and younger patients with hypertension: overview, meta-analyses and meta-regression analyses of randomized trials.J Hypertens. 2018 Aug;36(8):1622-1636. doi: 10.1097/HJH.0000000000001787. J Hypertens. 2018. PMID: 29847485 Review.
-
Antihypertensive Drug Deintensification and Recurrent Falls in Long-Term Care.Health Serv Res. 2018 Dec;53(6):4066-4086. doi: 10.1111/1475-6773.13074. Epub 2018 Oct 23. Health Serv Res. 2018. PMID: 30353536 Free PMC article.
-
Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults : A Retrospective Observational Study.Ann Intern Med. 2021 Dec;174(12):1666-1673. doi: 10.7326/M21-1456. Epub 2021 Oct 5. Ann Intern Med. 2021. PMID: 34606315 Free PMC article.
-
Effect of Intensive Blood Pressure Lowering on Cardiovascular Outcomes: A Systematic Review Prepared for the 2020 U.S. Department of Veterans Affairs/U.S. Department of Defense Guidelines.Ann Intern Med. 2020 Dec 1;173(11):895-903. doi: 10.7326/M20-2037. Epub 2020 Sep 1. Ann Intern Med. 2020. PMID: 32866419
Cited by
-
Effect of antihypertensive deprescribing on hospitalisation and mortality: long-term follow-up of the OPTiMISE randomised controlled trial.Lancet Healthy Longev. 2024 Aug;5(8):e563-e573. doi: 10.1016/S2666-7568(24)00131-4. Epub 2024 Jul 30. Lancet Healthy Longev. 2024. PMID: 39094592 Free PMC article. Clinical Trial.
-
Survival benefit and impact of adjuvant therapies following FOLFOX-HAIC-based conversion therapy with unresectable hepatocellular carcinoma: a retrospective cohort study.J Cancer Res Clin Oncol. 2023 Nov;149(16):14761-14774. doi: 10.1007/s00432-023-05243-7. Epub 2023 Aug 17. J Cancer Res Clin Oncol. 2023. PMID: 37589925 Free PMC article.
-
Systemic therapy with or without transcatheter intra-arterial therapies for unresectable hepatocellular carcinoma: a real-world, multi-center study.Front Immunol. 2023 Apr 26;14:1138355. doi: 10.3389/fimmu.2023.1138355. eCollection 2023. Front Immunol. 2023. PMID: 37180173 Free PMC article.
-
Antihypertensive Deprescribing in Older Adults: a Practical Guide.Curr Hypertens Rep. 2022 Nov;24(11):571-580. doi: 10.1007/s11906-022-01215-3. Epub 2022 Jul 26. Curr Hypertens Rep. 2022. PMID: 35881225 Free PMC article. Review.
-
Risk factors of undiagnosed and uncontrolled hypertension in primary care patients with hypertension: a cross-sectional study.BMC Prim Care. 2024 Aug 20;25(1):311. doi: 10.1186/s12875-024-02511-4. BMC Prim Care. 2024. PMID: 39164618 Free PMC article.
References
-
- Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887‐1898. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71:e127‐e248. - PubMed
