

Clinical outcomes of modifying hypertension treatment intensity in older adults treated to low blood pressure
- PMID: 34097300
- PMCID: PMC8497391
- DOI: 10.1111/jgs.17295
Clinical outcomes of modifying hypertension treatment intensity in older adults treated to low blood pressure
Abstract
Background/objectives: Hypertension treatment reduces cardiovascular events. However, uncertainty remains about benefits and harms of deintensification or further intensification of antihypertensive medication when systolic blood pressure (SBP) is tightly controlled in older multimorbid patients, because of their frequent exclusion in trials. We assessed the association of hypertension treatment deintensification or intensification with clinical outcomes in older adults with tightly controlled SBP.
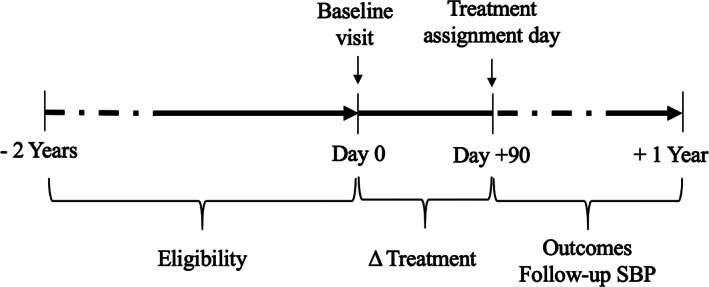
Design: Longitudinal cohort study (2011-2013) with 9-month follow-up.
Setting: U.S.-nationwide primary care Veterans Health Administration healthcare system.
Participants: Veterans aged 65 and older with baseline SBP <130 mmHg and ≥1 antihypertensive medication during ≥2 consecutive visits (N = 228,753).
Exposure: Deintensification or intensification, compared with stable treatment.
Main outcomes and measures: Cardiovascular events, syncope, or fall injury, as composite and distinct outcomes, within 9 months after exposure. Adjusted logistic regression and inverse probability of treatment weighting (IPTW, sensitivity analysis).
Results: Among 228,753 patients (mean age 75 [SD 7.5] years), the composite outcome occurred in 11,982/93,793 (12.8%) patients with stable treatment, 14,768/72,672 (20.3%) with deintensification, and 11,821/62,288 (19.0%) with intensification. Adjusted absolute outcome risk (95% confidence interval) was higher for deintensification (18.3% [18.1%-18.6%]) and intensification (18.7% [18.4%-19.0%]), compared with stable treatment (14.8% [14.6%-15.0%]), p < 0.001 for both effects in the multivariable model). Deintensification was associated with fewer cardiovascular events than intensification. At baseline SBP <95 mmHg, cardiovascular event risk was similar for deintensification and stable treatment, and fall risk lower for deintensification than intensification. IPTW yielded similar results. Mean follow-up SBP was 124.1 mmHg for stable treatment, 125.1 mmHg after deintensification (p < 0.001), and 124.0 mmHg after intensification (p < 0.001).
Conclusion: Antihypertensive treatment deintensification in older patients with tightly controlled SBP was associated with worse outcomes than continuing same treatment intensity. Given higher mortality among patients with treatment modification, confounding by indication may not have been fully corrected by advanced statistical methods for observational data analysis.
Keywords: Veterans; cardiovascular event; deintensification; elderly; fall injury; hypertension; intensification; syncope; treatment.
© 2021 The Authors. Journal of the American Geriatrics Society published by Wiley Periodicals LLC on behalf of The American Geriatrics Society.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures

References
-
- Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887‐1898. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71:e127‐e248. - PubMed
