

Asymptomatic Bordetella pertussis infections in a longitudinal cohort of young African infants and their mothers
- PMID: 34097599
- PMCID: PMC8184211
- DOI: 10.7554/eLife.65663
Asymptomatic Bordetella pertussis infections in a longitudinal cohort of young African infants and their mothers
Abstract
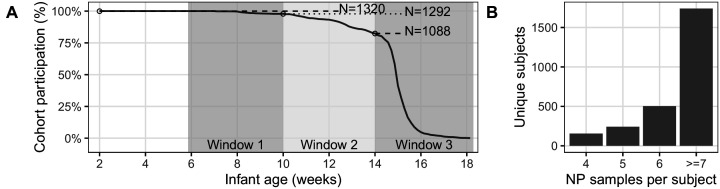
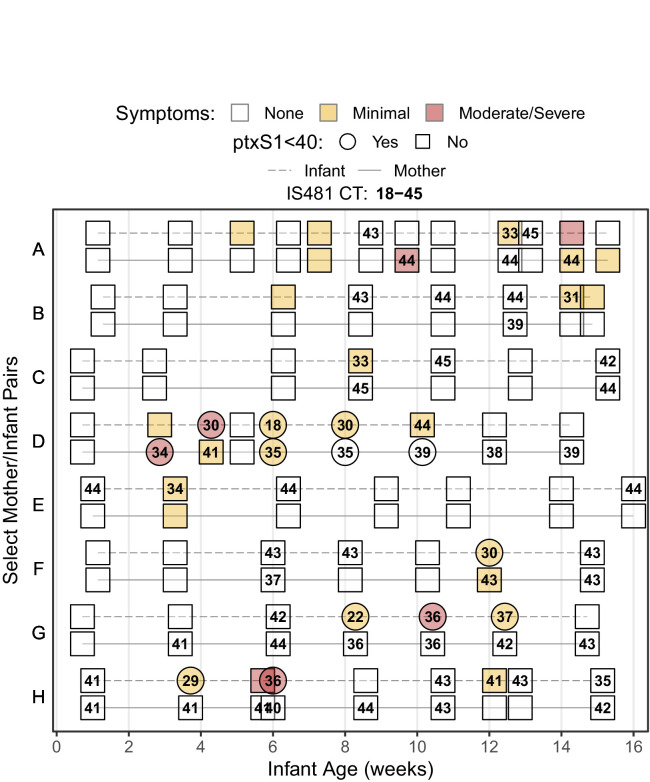
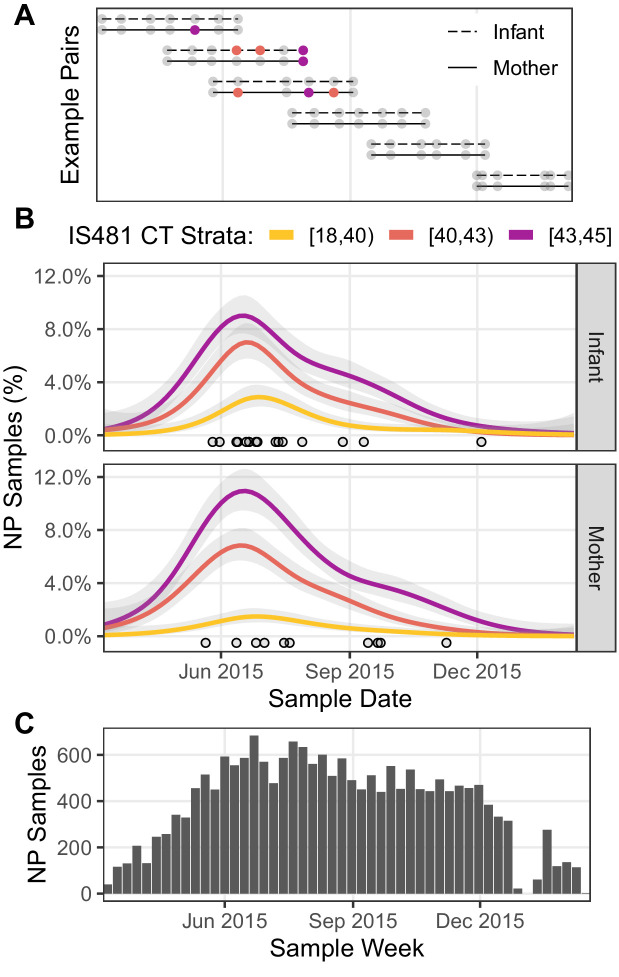
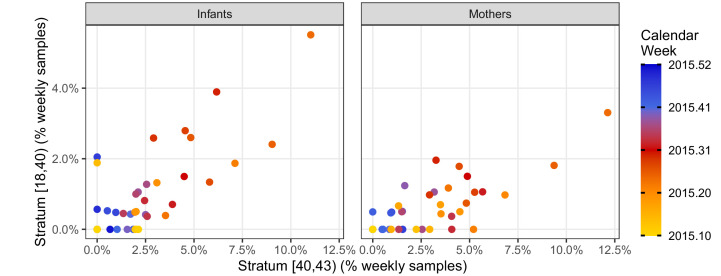
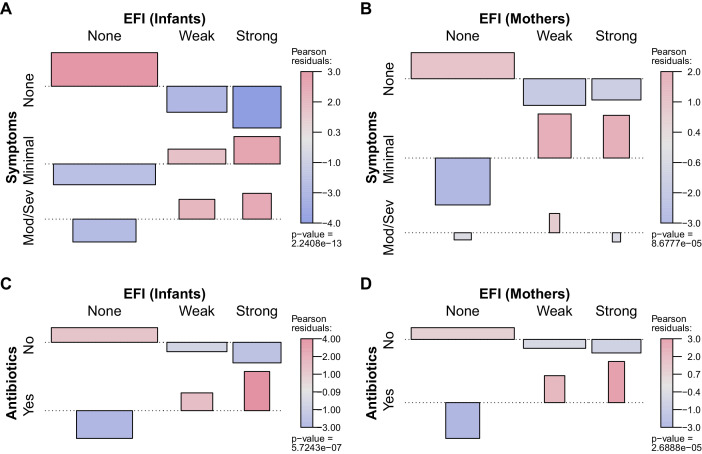
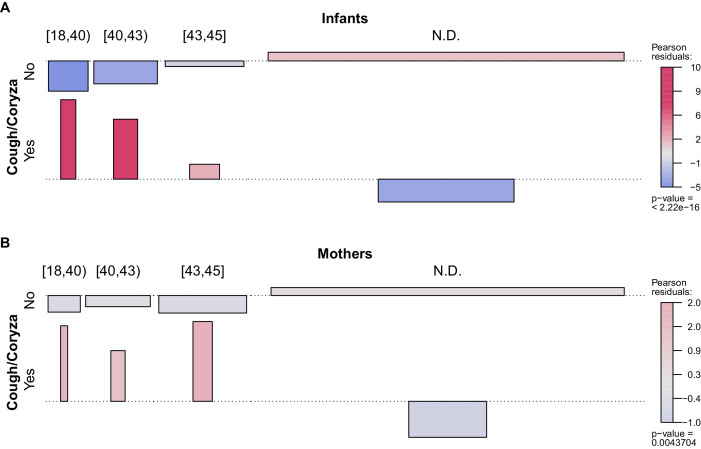
Recent pertussis resurgence in numerous countries may be driven by asymptomatic infections. Most pertussis surveillance studies are cross-sectional and cannot distinguish asymptomatic from pre-symptomatic infections. Longitudinal surveillance could overcome this barrier, providing more information about the true burden of pertussis at the population level. Here we analyze 17,442 nasopharyngeal samples from a longitudinal cohort of 1320 Zambian mother/infant pairs. Our analysis has two elements. First, we demonstrate that the full range of IS481 qPCR CT values provides insight into pertussis epidemiology, showing concordance of low and high CT results over time, within mother/infant pairs, and in relation to symptomatology. Second, we exploit these full-range qPCR data to demonstrate a high incidence of asymptomatic pertussis, including among infants. Our results demonstrate a wider burden of pertussis infection than we anticipated in this population, and expose key limitations of threshold-based interpretation of qPCR results in infectious disease surveillance.
Keywords: Africa; Bordetella pertussis; asymptomatic infection; cohort study; epidemiology; global health; human; qPCR; whooping cough.
© 2021, Gill et al.
Conflict of interest statement
CG, CG, WM, LM, DT, RP, GK, ZM, PR No competing interests declared
Figures
References
-
- Armangil D, Tekinalp G, Yurdakök M, Yalçin E. Maternal pertussis is hazardous for a newborn: a case report. The Turkish Journal of Pediatrics. 2010;52:206–210. - PubMed
-
- Bolotin S, Quinn H, McIntyre P. Epilogue. In: Rohani P, Scarpino S. V, editors. Pertussis: Epidemiology, Immunology and Evolution. Oxford University Press; 2018. pp. 1–2. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
