

Rapid versus standard antimicrobial susceptibility testing to guide treatment of bloodstream infection
- PMID: 34097767
- PMCID: PMC8561756
- DOI: 10.1002/14651858.CD013235.pub2
Rapid versus standard antimicrobial susceptibility testing to guide treatment of bloodstream infection
Abstract
Background: Rapid antimicrobial susceptibility tests are expected to reduce the time to clinically important results of a blood culture. This might enable clinicians to better target therapy to a person's needs, and thereby, improve health outcomes (mortality, length of hospital stay), and reduce unnecessary prescribing of broad-spectrum antibiotics; thereby reducing antimicrobial resistance rates.
Objectives: To assess the effects of rapid susceptibility testing versus standard susceptibility testing for bloodstream infections (BSIs).
Search methods: To identify studies with selected outcomes, we searched the Cochrane Infectious Diseases Group Specialised Register, CENTRAL, MEDLINE, LILACS, and two trials registries, between 1987 and October 2020. We used 'bloodstream infection' and 'antimicrobial susceptibility tests' as search terms. We had no language or publication status limitations.
Selection criteria: Randomized controlled trials (RCTs) comparing rapid antimicrobial susceptibility testing (with a time-to-result of ≤ 8 hours) versus conventional antimicrobial susceptibility testing in people with a BSI caused by any bacteria, as identified by a positive blood culture.
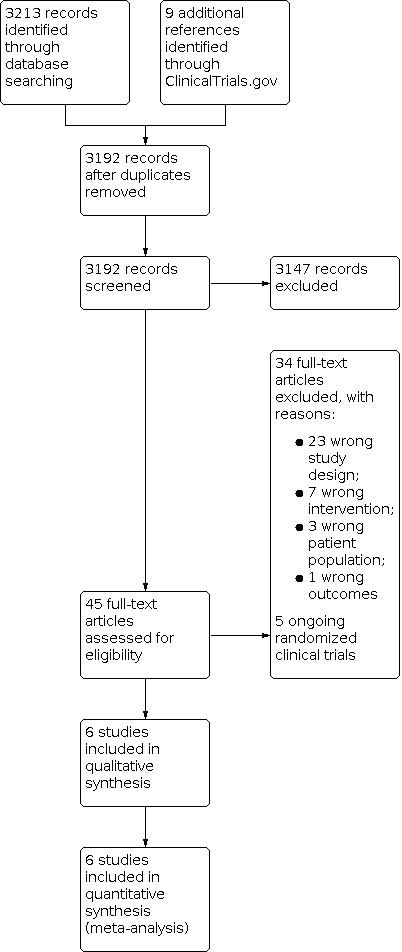
Data collection and analysis: Two review authors independently screened references, full-text reports of potentially relevant studies, extracted data from the studies, and assessed risk of bias. Any disagreement was discussed and resolved with a third review author. For mortality, a dichotomous outcome, we extracted the number of events in each arm, and presented a risk ratio (RR) with 95% confidence interval (CI) to compare rapid susceptibility testing to conventional methods. We used Review Manager 5.4 to meta-analyse the data. For other outcomes, which are time-to-event outcomes (time-to-discharge from hospital, time-to-first appropriate antibiotic change), we conducted qualitative narrative synthesis, due to heterogeneity of outcome measures. MAIN RESULTS: We included six trials, with 1638 participants. For rapid antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.10, 95% CI 0.82 to 1.46; 6 RCTs, 1638 participants; low-certainty evidence). In subgroup analysis, for rapid genotypic or molecular antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.02, 95% CI 0.69 to 1.49; 4 RCTs, 1074 participants; low-certainty evidence). For phenotypic rapid susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.37, 95% CI 0.80 to 2.35; 2 RCTs, 564 participants; low-certainty evidence). In qualitative analysis, rapid susceptibility testing may make little or no difference in time-to-discharge (4 RCTs, 1165 participants; low-certainty evidence). In qualitative analysis, rapid genotypic susceptibility testing compared to conventional testing may make little or no difference in time-to-appropriate antibiotic (3 RCTs, 929 participants; low-certainty evidence). In subgroup analysis, rapid phenotypic susceptibility testing compared to conventional testing may improve time-to-appropriate antibiotic (RR -17.29, CI -45.05 to 10.47; 2 RCTs, 564 participants; low-certainty evidence). AUTHORS' CONCLUSIONS: The theoretical benefits of rapid susceptibility testing have not been demonstrated to directly improve mortality, time-to-discharge, or time-to-appropriate antibiotic in these randomized studies. Future large prospective studies should be designed to focus on the most clinically meaningful outcomes, and aim to optimize blood culture pathways.
บทนำ: การทดสอบความไวต่อยาต้านจุลชีพอย่างรวดเร็วคาดว่าจะช่วยลดเวลาในการให้ผลลัพธ์ที่สำคัญทางคลินิกของการเพาะเชื้อจากเลือด สิ่งนี้อาจช่วยให้แพทย์สามารถกำหนดเป้าหมายการรักษาตามความต้องการของบุคคลได้ดีขึ้น และด้วยเหตุนี้จึงปรับปรุงผลด้านสุขภาพ (อัตราการเสียชีวิต ระยะเวลาการพักรักษาตัวในโรงพยาบาล) และลดการสั่งจ่ายยาปฏิชีวนะครอบคลุมกว้างโดยไม่จำเป็น จึงช่วยลดอัตราการดื้อยาต้านจุลชีพ วัตถุประสงค์: เพื่อประเมินผลของการทดสอบความไวอย่างรวดเร็วเทียบกับการทดสอบความไวแบบมาตรฐานสำหรับการติดเชื้อในกระแสเลือด (BSIs) วิธีการสืบค้น: เพื่อค้นหาการศึกษาสำหรับผลลัพธ์ที่เลือกเราได้สืบค้น Cochrane Infectious Diseases Group Specialised Register, CENTRAL, MEDLINE, LILACS และ trial registries 2 แหล่ง ระหว่างปี 1987 ถึงตุลาคม 2020 เราใช้ 'bloodstream infection' และ 'antimicrobial susceptibility tests' เป็นคำค้นหา เราไม่ใช้ข้อจำกัดด้านภาษาหรือสถานะการตีพิมพ์ เกณฑ์การคัดเลือก: การทดลองแบบสุ่มที่มีกลุ่มควบคุม (RCTs) เปรียบเทียบการทดสอบความไวต่อยาต้านจุลชีพอย่างรวดเร็ว (โดยใช้เวลาถึงผลลัพธ์ ≤ 8 ชั่วโมง) เทียบกับการทดสอบความไวต่อยาต้านจุลชีพแบบเดิมในผู้ที่มี BSI ที่เกิดจากแบคทีเรียใด ๆ ตามที่พบโดยการเพาะเชื้อในเลือดที่เป็นบวก การรวบรวมและวิเคราะห์ข้อมูล: ผู้ประพันธ์การทบทวนวรรณกรรม 2 คนคัดกรองเอกสารอ้างอิง รายงานฉบับเต็มของการศึกษาที่อาจเกี่ยวข้อง คัดลอกข้อมูลจากการศึกษาและประเมินความเสี่ยงของอคติอย่างอิสระต่อกัน กรณีมีความเห็นไม่ตรงกันได้มีการการสนทนากับผู้ประพันธ์การทบทวนวรรณกรรมคนที่ 3 สำหรับการเสียชีวิต dichotomous outcome เราได้คัดลอกจำนวนเหตุการณ์ในแต่ละกลุ่ม และนำเสนอ risk ratio (RR) และช่วงความเชื่อมั่น 95% (CI) เพื่อเปรียบเทียบการทดสอบความไวอย่างรวดเร็วกับวิธีการทั่วไป เราใช้ Review Manager 5.4 ในการวิเคราะห์ข้อมูล สำหรับผลลัพธ์อื่นๆ ซึ่งเป็นผลลัพธ์แบบ time‐to‐event (ระยะเวลาในการจำหน่ายจากโรงพยาบาล การเปลี่ยนยาปฏิชีวนะที่เหมาะสมครั้งแรก) เราได้ทำการสังเคราะห์เชิงคุณภาพแบบบรรยายเนื่องจากผลลัพธ์ที่แตกต่างกัน ผลการวิจัย: เรารวมการทดลอง 6 รายการ โดยมีผู้เข้าร่วม 1638 คน สำหรับการทดสอบความไวต่อยาต้านจุลชีพอย่างรวดเร็วเมื่อเทียบกับวิธีการทั่วไป พบว่าการตายระหว่างกลุ่มมีความแตกต่างกันเล็กน้อยหรือไม่มี (RR 1.10, 95% CI 0.82 ถึง 1.46; 6 RCTs, ผู้เข้าร่วม 1638 คน; หลักฐานมีความเชื่อมั่นในระดับต่ำ) ในการวิเคราะห์กลุ่มย่อยสำหรับการทดสอบความไวต่อยาต้านจุลชีพแบบ genotypic หรือ molecular อย่างรวดเร็ว เมื่อเทียบกับวิธีการทั่วไปพบว่า การตายระหว่างกลุ่มมีความแตกต่างกันเพียงเล็กน้อยหรือไม่มี (RR 1.02, 95% CI 0.69 ถึง 1.49; 4 RCTs, ผู้เข้าร่วม 1074 คน; หลักฐานมีความเชื่อมั่นในระดับต่ำ) สำหรับการทดสอบความไวอย่างรวดเร็วแบบ Phenotypic เมื่อเทียบกับวิธีการทั่วไปพบว่า การตายระหว่างกลุ่มมีความแตกต่างกันเล็กน้อยหรือไม่มี (RR 1.37, 95% CI 0.80 ถึง 2.35; 2 RCTs, ผู้เข้าร่วม 564 คน; หลักฐานมีความเชื่อมั่นในระดับต่ำ) ในการวิเคราะห์เชิงคุณภาพ การทดสอบความไวอย่างรวดเร็วอาจสร้างความแตกต่างเพียงเล็กน้อยหรือไม่มีความแตกต่าง ในเวลาถึงการออกจากโรงพยาบาล (4 RCTs, ผู้เข้าร่วม 1165 คน; หลักฐานมีความเชื่อมั่นในระดับต่ำ) ในการวิเคราะห์เชิงคุณภาพ การทดสอบความไวอย่างรวดเร็วแบบ Genotypic เมื่อเทียบกับการทดสอบแบบเดิมอาจสร้างความแตกต่างเพียงเล็กน้อยหรือไม่มี ในเวลาถึงการให้ยาปฏิชีวนะที่เหมาะสม (3 RCTs, ผู้เข้าร่วม 929 คน; หลักฐานมีความเชื่อมั่นในระดับต่ำ) ในการวิเคราะห์กลุ่มย่อย การทดสอบความไวอย่างรวดเร็วแบบ Phenotypic เมื่อเทียบกับการทดสอบแบบเดิมอาจช่วยปรับปรุงเวลาถึงการให้ยาปฏิชีวนะที่เหมาะสม (RR ‐17.29, CI ‐45.05 ถึง 10.47; 2 RCTs, ผู้เข้าร่วม 564 คน; หลักฐานมีความเชื่อมั่นในระดับต่ำ) ข้อสรุปของผู้วิจัย: ผลประโยชน์ทางทฤษฎีของการทดสอบความไวอย่างรวดเร็วไม่ได้แสดงให้เห็นโดยตรงในการปรับปรุงอัตราการตาย เวลาถึงการออกจากโรงพยาบาล หรือเวลาถึงการให้ยาปฏิชีวนะที่เหมาะสมในการศึกษาแบบสุ่มเหล่านี้ การศึกษาแบบไปข้างหน้าในอนาคตที่มีขนาดใหญ่ควรได้รับการออกแบบมาเพื่อมุ่งเน้นไปที่ผลลัพธ์ที่มีความหมายทางคลินิกมากที่สุด และมีจุดมุ่งหมายเพื่อเพิ่มประสิทธิภาพเส้นทางการเพาะเลี้ยงเชื้อในเลือด.
Antecedentes: Se espera que las pruebas rápidas de susceptibilidad antimicrobiana reduzcan el tiempo de obtención de resultados clínicamente importantes de un hemocultivo. Esto podría permitir a los médicos orientar mejor el tratamiento a las necesidades de la persona y, por tanto, mejorar los desenlaces de salud (mortalidad, duración de la estancia hospitalaria) y reducir la prescripción innecesaria de antibióticos de amplio espectro, con lo que se reducirían las tasas de farmacorresistencia.
Objetivos: Evaluar los efectos de las pruebas rápidas de susceptibilidad versus las pruebas estándares de susceptibilidad para la septicemia. MÉTODOS DE BÚSQUEDA: Para identificar estudios con los desenlaces seleccionados se realizaron búsquedas en el Registro especializado del Grupo Cochrane de Enfermedades infecciosas (Cochrane Infectious Diseases Group), CENTRAL, MEDLINE, LILACS y en dos registros de ensayos, entre 1987 y octubre de 2020. Se utilizaron como términos de búsqueda "bloodstream infection" y "antimicrobial susceptibility tests". No se aplicaron límites de idioma ni de estado de publicación. CRITERIOS DE SELECCIÓN: Ensayos controlados aleatorizados (ECA) que comparan las pruebas rápidas de susceptibilidad antimicrobiana (con un tiempo de obtención de los resultados de ≤ 8 horas) versus las pruebas convencionales de susceptibilidad antimicrobiana en personas con una septicemia causada por cualquier bacteria, identificada por un hemocultivo positivo. OBTENCIÓN Y ANÁLISIS DE LOS DATOS: Dos autores de la revisión examinaron de forma independiente las referencias, los informes de texto completo de los estudios potencialmente relevantes, extrajeron los datos de los estudios y evaluaron el riesgo de sesgo. Cualquier desacuerdo se debatió y se resolvió con un tercer autor de la revisión. Para la mortalidad, un desenlace dicotómico, se extrajo el número de eventos en cada grupo, y se presentó una razón de riesgos (RR) con un intervalo de confianza (IC) del 95% para comparar las pruebas rápidas de susceptibilidad con los métodos convencionales. Para realizar los metanálisis de los datos se utilizó Review Manager 5.4. Para otros desenlaces, que son desenlaces de tiempo hasta el evento (tiempo transcurrido hasta el alta hospitalaria, tiempo transcurrido hasta el primer cambio apropiado de antibiótico), se realizó una síntesis narrativa cualitativa debido a la heterogeneidad de las medidas de desenlace.
Resultados principales: Se incluyeron seis ensayos con 1638 participantes. En el caso de las pruebas rápidas de susceptibilidad antimicrobiana comparadas con los métodos convencionales, hubo poca o ninguna diferencia en la mortalidad entre los grupos (RR 1,10; IC del 95%: 0,82 a 1,46; seis ECA, 1638 participantes; evidencia de certeza baja). En el análisis de subgrupos, para las pruebas rápidas de susceptibilidad antimicrobiana genotípicas o moleculares en comparación con los métodos convencionales, hubo poca o ninguna diferencia en la mortalidad entre los grupos (RR 1,02; IC del 95%: 0,69 a 1,49; cuatro ECA, 1074 participantes; evidencia de certeza baja). En el caso de las pruebas rápidas de susceptibilidad fenotípicas en comparación con los métodos convencionales hubo poca o ninguna diferencia en la mortalidad entre los grupos (RR 1,37; IC del 95%: 0,80 a 2,35; dos ECA, 564 participantes; evidencia de certeza baja). En el análisis cualitativo, las pruebas rápidas de susceptibilidad podrían suponer una diferencia escasa o nula en el tiempo transcurrido hasta el alta (cuatro ECA, 1165 participantes; evidencia de certeza baja). En el análisis cualitativo, las pruebas rápidas de susceptibilidad genotípicas comparadas con las pruebas convencionales podrían suponer una diferencia escasa o nula en el tiempo transcurrido hasta recibir el antibiótico apropiado (tres ECA, 929 participantes; evidencia de certeza baja). En el análisis de subgrupos, las pruebas rápidas de susceptibilidad fenotípicas comparadas con las pruebas convencionales podrían mejorar el tiempo transcurrido hasta recibir el antibiótico apropiado (RR ‐17,29; IC: ‐45,05 a 10,47; dos ECA, 564 participantes; evidencia de certeza baja).
Conclusiones de los autores: Los beneficios teóricos de las pruebas rápidas de susceptibilidad no han mostrado mejorar directamente la mortalidad, el tiempo transcurrido hasta el alta ni el tiempo transcurrido hasta recibir el antibiótico apropiado en estos estudios aleatorizados. Los estudios prospectivos futuros de gran envergadura se deben diseñar para centrarse en los desenlaces más importantes desde el punto de vista clínico y tener como objetivo optimizar las vías de hemocultivo.
Copyright © 2021 The Authors. Cochrane Database of Systematic Reviews published by John Wiley & Sons, Ltd. on behalf of The Cochrane Collaboration.
Conflict of interest statement
VA has no known conflicts of interest.
PH was previously employed full‐time by Cochrane Infectious Diseases Group (CIDG), and currently works full‐time within the UK National Health Service (NHS). He received a Registration Scholarship to attend the 23rd Annual British HIV Association Conference 2017 from ViiV healthcare. ViiV had no involvement in the selection of recipients of the scholarship. In 2018, he attended a CPD‐certified clinical research training programme, organized and funded by Gilead Sciences Europe Ltd. To the best of his knowledge, neither financial or non‐financial conflicts of interests have influenced the current submitted work.
SK is a scientific advisor and shareholder in QuantuMDx, a company that is developing rapid diagnostic tests for several infections, and is a scientific advisor to Foundation for Innovative New Diagnostics (FIND). The opinions in this review are personal opinions, and do not represent views of either organization.
MC has no known conflicts of interest.
TP is the clinical lead of a NHS diagnostic microbiology laboratory at South West London Pathology. He is on advisory boards for Roche, Pfizer, and Singulex for diagnostics.
Figures







Update of
- doi: 10.1002/14651858.CD013235
Similar articles
-
Early discontinuation of antibiotics for febrile neutropenia versus continuation until neutropenia resolution in people with cancer.Cochrane Database Syst Rev. 2019 Jan 3;1(1):CD012184. doi: 10.1002/14651858.CD012184.pub2. Cochrane Database Syst Rev. 2019. PMID: 30605229 Free PMC article.
-
Standard versus biofilm antimicrobial susceptibility testing to guide antibiotic therapy in cystic fibrosis.Cochrane Database Syst Rev. 2020 Jun 10;6(6):CD009528. doi: 10.1002/14651858.CD009528.pub5. Cochrane Database Syst Rev. 2020. PMID: 32520436 Free PMC article.
-
Interventions for bacterial folliculitis and boils (furuncles and carbuncles).Cochrane Database Syst Rev. 2021 Feb 26;2(2):CD013099. doi: 10.1002/14651858.CD013099.pub2. Cochrane Database Syst Rev. 2021. PMID: 33634465 Free PMC article.
-
Antibiotics for trachoma.Cochrane Database Syst Rev. 2019 Sep 26;9(9):CD001860. doi: 10.1002/14651858.CD001860.pub4. Cochrane Database Syst Rev. 2019. PMID: 31554017 Free PMC article.
-
Chlorhexidine bathing of the critically ill for the prevention of hospital-acquired infection.Cochrane Database Syst Rev. 2019 Aug 30;8(8):CD012248. doi: 10.1002/14651858.CD012248.pub2. Cochrane Database Syst Rev. 2019. PMID: 31476022 Free PMC article.
Cited by
-
Response to Author Comments on "Clinical, microbiological characteristics and predictors of mortality in patients with carbapenemase-producing Enterobacterales blood stream infections".Infect Prev Pract. 2023 Nov 17;5(4):100327. doi: 10.1016/j.infpip.2023.100327. eCollection 2023 Dec. Infect Prev Pract. 2023. PMID: 38107238 Free PMC article. No abstract available.
-
Direct Identification, Antimicrobial Susceptibility Testing, and Extended-Spectrum β-Lactamase and Carbapenemase Detection in Gram-Negative Bacteria Isolated from Blood Cultures.Infect Drug Resist. 2022 Apr 6;15:1587-1599. doi: 10.2147/IDR.S350612. eCollection 2022. Infect Drug Resist. 2022. PMID: 35418761 Free PMC article.
-
Impact of a Laboratory-Developed Phenotypic Rapid Susceptibility Test Directly From Positive Blood Cultures on Time to Narrowest Effective Therapy in Patients With Gram-Negative Bacteremia: A Prospective Randomized Trial.Open Forum Infect Dis. 2022 Jul 22;9(7):ofac347. doi: 10.1093/ofid/ofac347. eCollection 2022 Jul. Open Forum Infect Dis. 2022. PMID: 35919072 Free PMC article.
-
Bloodstream Infections: Comparison of Diagnostic Methods and Therapeutic Consequences between a Hospital in a Resource-Limited Setting and Two French Hospitals.Microorganisms. 2023 Aug 23;11(9):2136. doi: 10.3390/microorganisms11092136. Microorganisms. 2023. PMID: 37763979 Free PMC article.
-
Evaluating the impact of rapid antimicrobial susceptibility testing for bloodstream infections: a review of actionability, antibiotic use and patient outcome metrics.J Antimicrob Chemother. 2024 Sep 19;79(12 Suppl 2):i13-i25. doi: 10.1093/jac/dkae282. J Antimicrob Chemother. 2024. PMID: 39298359 Free PMC article. Review.
References
References to studies included in this review
Allaouchiche 1999 {published data only}
-
- Allaouchiche B, Jaumain H, Zambardi G, Chassard D, Freney J. Clinical impact of rapid oxacillin susceptibility testing using a PCR assay in Staphylococcus aureus bactaeremia. Journal of Infection 1999;39(3):198-204. - PubMed
Banerjee 2015 {published data only}
-
- NCT01898208. Rapid identification and susceptibility testing of pathogens from blood cultures. www.clinicaltrials.gov/ct2/show/NCT01898208 (last update posted 15 March 2016).
Banerjee 2020 {published and unpublished data}
-
- Banarjee R, Komarow L, Virk A, Rajapakse NS, Schuetz A, Dylla B, et al. Randomized trial evaluating clinical impact of RAPid IDentification and Susceptibility testing for Gram Negative bacteremia (RAPIDS-GN). Clinical Infectious Diseases 2020 May 7 [Epub ahead of print];ciaa528. [DOI: 10.1093/cid/ciaa528] - DOI - PMC - PubMed
Beuving 2015 {published data only}
-
- Beuving J, Wolffs PF, Hansen WL, Stobberingh EE, Bruggeman CA, Kessels A, et al. Impact of same-day antibiotic susceptibility testing on time to appropriate antibiotic treatment of patients with bacteraemia: a randomised controlled trial. European Journal of Clinical Microbiology & Infectious Diseases 2015;34(4):831-8. - PubMed
Emonet 2015 {published data only}
-
- Emonet S, Charles PG, Harbarth S, Renzi G, Cherkaoui A, Rougemont M, et al. Rapid molecular diagnosis using femA mecA real-time PCR for staphylococcal bacteraemia improves early appropriate antibiotic prescribing: a randomised clinical trial. Antimicrobial Resistance & Infection Control 2015;4(Suppl 1):O1.
-
- Emonet S, Charles PG, Harbarth S, Stewardson AJ, Renzi G, Uckay I, et al. Rapid molecular determination of methicillin resistance in staphylococcal bacteraemia improves early targeted antibiotic prescribing: a randomized clinical trial. Clinical Microbiology and Infection 2016;22(11):946.e9‐15. - PubMed
Kim 2021 {published data only}
-
- Kim JH, Kim I, Kang CK, Jun KI, Yoo SH, Chun JY, et al. Enhanced antimicrobial stewardship based on rapid phenotypic antimicrobial susceptibility testing for bacteraemia in patients with haematological malignancies: a randomized controlled trial. Clinical Microbiology and Infection 2021;27(1):69-75. [DOI: 10.1016/j.cmi.2020.03.038.] - DOI - PubMed
-
- NCT03611257. Effect of dRAST on treatment for bacteremia in patients with hematologic diseases. www.clinicaltrials.gov/ct2/show/NCT03611257 (first posted 2 August 2018).
References to studies excluded from this review
Bloos 2010 {published data only}
-
- Bloos F, Hinder F, Becker K, Sachse S, Dessap AM, Straube E, et al. A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis. Intensive Care Medicine 2010;36(2):241-7. - PubMed
Bookstaver 2017 {published data only}
-
- Bookstaver PB, Nimmich EB, Smith TJ, Justo JA, Kohn J, Hammer KL, et al. Cumulative effect of an antimicrobial stewardship and rapid diagnostic testing bundle on early streamlining of antimicrobial therapy in gram-negative bloodstream infections. Antimicrobial Agents and Chemotherapy 2017;61(9):pii: e00189-17. - PMC - PubMed
Box 2015 {published data only}
-
- Box MJ, Sullivan EL, Ortwine KN, Parmenter MA, Quigley MM, Aguilar-Higgins LM, et al. Outcomes of rapid identification for gram-positive bacteremia in combination with antibiotic stewardship at a community-based hospital system. Pharmacotherapy 2015;35(3):269-76. - PubMed
Bruins 2005 {published data only}
-
- Bruins M, Oord H, Bloembergen P, Wolfhagen M, Casparie A, Degener J, et al. Lack of effect of shorter turnaround time of microbiological procedures on clinical outcomes: a randomised controlled trial among hospitalised patients in the Netherlands. European Journal of Clinical Chemistry and Clinical Biochemistry 2005;24(5):305-13. - PubMed
Burnham 2019 {published data only}
-
- Burnham JP, Wallace MA, Fuller BM, Shupe A, Burnham CD, Kollef MH. Clinical effect of expedited pathogen identification and susceptibility testing for gram-negative bacteremia and candidemia by use of the accelerate pheno™ system. Journal of Applied Laboratory Medicine 2019;3(4):569-79. - PubMed
Buss 2018 {published data only}
Cambau 2017 {published data only}
-
- Cambau E, Durand-Zaleski I, Bretagne S, Brun-Buisson C, Cordonnier C, Duval X, et al. Performance and economic evaluation of the molecular detection of pathogens for patients with severe infections: the EVAMICA open-label, cluster-randomised, interventional crossover trial. Intensive Care Medicine 2017;43(11):1613-25. - PMC - PubMed
Chan, 2009 {published data only}
-
- Chan KY, Lam HS, Cheung HM, Chan AK, Li K. Rapid identification and differentiation of gram-negative and gram-positive bacterial bloodstream infections by quantitative polymerase chain reaction in preterm infants. Critical Care Medicine 2009;37(8):2441-7. - PubMed
Clerc 2014 {published data only}
-
- Clerc O, Prod'hom G, Senn L, Jaton K, Zanetti G, Calandra T, et al. Matrix-assisted laser desorption ionization time-of-flight mass spectrometry and PCR-based rapid diagnosis of Staphylococcus aureus bacteraemia. Clinical Microbiology and Infection 2014;20(4):355-60. - PubMed
Cosgrove 2016 {published data only}
-
- Cosgrove SE, Li DX, Tamma PD, Avdic E, Hadhazy E, Wakefield T, et al. Use of PNA FISH for blood cultures growing gram-positive cocci in chains without a concomitant antibiotic stewardship intervention does not improve time to appropriate antibiotic therapy. Diagnostic Microbiology and Infectious Disease 2016;86(1):86-92. - PubMed
Doern 1994 {published data only}
Draz 2013 {published data only}
Ehren 2019 {published data only}
-
- Ehren K, Meissner A, Jazmati N, Wille J, Jung N, Vehreschild JJ, et al. Clinical impact of rapid species identification from positive blood cultures with same-day phenotypic antimicrobial susceptibility testing on the management and outcome of bloodstream infections. Clinical Infectious Diseases 2020;70(7):1285-93. - PubMed
Farfour 2019 {published data only}
-
- Farfour E, Si Larbi AG, Cardot E, Limousin L, Mathonnet D, Cahen P, et al. Impact of rapid diagnostic tests on the management of patients presenting with Enterobacteriaceae bacteremia. Medecine et Maladies Infectieuses 2019;49(3):202-7. - PubMed
Garcia‐Vazquez 2013 {published data only}
-
- Garcia-Vazquez E, Moral-Escudero E, Hernandez-Torres A, Canteras M, Gomez J, Ruiz J. What is the impact of a rapid diagnostic E-test in the treatment of patients with gram-negative bacteraemia? Scandinavian Journal of Infectious Diseases 2013;45(8):623-8. - PubMed
Garnier 2019 {published data only}
-
- Garnier M, Gallah S, Vimont S, Benzerara Y, Labbe V, Constant AL, et al. Multicentre randomised controlled trial to investigate usefulness of the rapid diagnostic betaLACTA test performed directly on bacterial cell pellets from respiratory, urinary or blood samples for the early de-escalation of carbapenems in septic intensive care unit patients: the BLUE-CarbA protocol. BMJ Open 2019;9(2):e024561. - PMC - PubMed
Grijalva 2020 {published data only}
-
- Grijalva M, De La Torre K, Sánchez N. The clinical impact of a multiplex real-time PCR system for microbiological diagnosis of sepsis: a mortality study. New Microbiologica 2020;43(2):64-9. [PMID: ] - PubMed
Idelevich 2015 {published data only}
-
- Idelevich EA, Silling G, Niederbracht Y, Penner H, Sauerland MC, Tafelski S, et al. Impact of multiplex PCR on antimicrobial treatment in febrile neutropenia: a randomized controlled study. Medical Microbiology and Immunology 2015;204(5):585-92. - PubMed
Jeyaratnam 2008 {published data only}
Kerremans 2008 {published data only}
-
- Kerremans JJ, Verboom P, Stijnen T, Hakkaart-van Roijen L, Goessens W, Verbrugh HA, et al. Rapid identification and antimicrobial susceptibility testing reduce antibiotic use and accelerate pathogen-directed antibiotic use. Journal of Antimicrobial Chemotherapy 2008;61(2):428-35. - PubMed
Koncelik 2016 {published data only}
-
- Koncelik DL, Hernandez J. The impact of implementation of rapid QuickFISH testing for detection of coagulase-negative staphylococci at a community-based hospital. American Journal of Clinical Pathology 2016;145(1):69-74. - PubMed
Lucignano 2011 {published data only}
Ly 2008 {published data only}
MacGowan 2020 {published data only}
May 2015 {published data only}
-
- May LS, Rothman RE, Miller LG, Brooks G, Zocchi M, Zatorski C, et al. A randomized clinical trial comparing use of rapid molecular testing for Staphylococcus aureus for patients with cutaneous abscesses in the emergency department with standard of care. Infection Control and Hospital Epidemiology 2015;36(12):1423-30. - PMC - PubMed
Naucler 2020 {published data only}
-
- Nauclér P, Huttner A, van Werkhoven CH, Singer M, Tattevin P, Einav S, et al. Impact of time to antibiotic therapy on clinical outcome in patients with bacterial infections in the emergency department: implications for antimicrobial stewardship. Clinical Microbiology and Infection 2020;20:1198-743. [DOI: 10.1016/j.cmi.2020.02.032] - DOI - PubMed
Pilmis 2019 {published data only}
-
- Pilmis B, Thy M, Diep J, Krob S, Perillaud C, Couzigou C, et al. Clinical impact of rapid susceptibility testing on MHR-SIR directly from blood cultures. Journal of Antimicrobial Chemotherapy 2019;74(10):3063-8. - PubMed
Rodrigues 2013 {published data only}
-
- Rodrigues C, Dos Santos MS, Filho HHC, Charbel CE, De Carvalho Sarahyba da Silva L, Rossi F, et al. Rapid molecular test (SeptiFast) reduced time for adjustment of antibiotic treatment in comparison with conventional blood cultures in critically ill sepsis patients: a randomized controlled clinical trial (preliminary results). Critical Care 2013;17(Suppl 4):P26.
Rodrigues 2019 {published data only}
Roshdy 2015 {published data only}
-
- Roshdy DG, Tran A, LeCroy N, Zeng D, Ou FS, Daniels LM, et al. Impact of a rapid microarray-based assay for identification of positive blood cultures for treatment optimization for patients with streptococcal and enterococcal bacteremia. Journal of Clinical Microbiology 2015;53(4):1411-4. - PMC - PubMed
Shang 2005 {published data only}
-
- Shang S, Chen G, Wu Y, Du L, Zhao Z. Rapid diagnosis of bacterial sepsis with PCR amplification and microarray hybridization in 16S rRNA gene. Pediatric Research 2005;58(1):143-8. - PubMed
Suzuki 2015 {published data only}
-
- Suzuki H, Hitomi S, Yaguchi Y, Tamai K, Ueda A, Kamata K, et al. Prospective intervention study with a microarray-based, multiplexed, automated molecular diagnosis instrument (Verigene system) for the rapid diagnosis of bloodstream infections, and its impact on the clinical outcomes. Journal of Infection and Chemotherapy 2015;21(12):849-56. - PubMed
Trenholme 1989 {published data only}
References to ongoing studies
ChiCTR2000034973 {published data only}
-
- ChiCTR2000034973. Clinical research of early rapid pathogen identification strategy for sepsis. chictr.org.cn/hvshowproject.aspx?id=44958 (last refreshed 26 July 2020).
NCT03744728 {published data only}
-
- NCT03744728. Randomized trial of fast bacterial identification and phenotypic antimicrobial susceptibility testing in patients with positive blood cultures using the Accelerate PhenoTest™ BC kit, performed on the Accelerate Pheno™ System as compared with the Verigene® BC-GP/GN. clinicaltrials.gov/ct2/show/NCT03744728 (first posted 16 November 2018).
NCT03745014 {published data only}
-
- NCT03745014. Clinical impact of fast phenotypic antimicrobial susceptibility testing on patients with Gram-negative rod bacteremia. clinicaltrials.gov/ct2/show/NCT03745014 (first posted 19 November 2018).
NCT03876990 {published data only}
-
- NCT03876990. Clinical and medico-economic evaluation of a rapid test (ePlex-BCID®, GenMark) for the diagnosis of bacteremia and fungemia (HEMOFAST). clinicaltrials.gov/ct2/show/NCT03876990?cond=NCT03876990 (first posted 15 March 2019).
NCT04153682 {published data only}
-
- NCT04153682. Trial on a strategy combining rapid diagnostic testing and antimicrobial stewardship to improve antibiotic use in patients with hospital-acquired pneumonia (SHARP). clinicaltrials.gov/ct2/show/NCT04153682 (first posted 6 November 2019).
Additional references
Balshem 2011
-
- Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. Journal of Clinical Epidemiology 2011;54(4):401-6. - PubMed
Baron 2013
-
- Baron EJ, Miller JM, Weinstein MP, Richter SS, Gilligan PH, Thomson RB Jr, et al. A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2013 recommendations by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM) a. Clinical Infectious Diseases 2013;57(4):e22-e121. - PMC - PubMed
Buehler 2015
-
- Buehler SS, Madison B, Snyder SR, Derzon JH, Cornish NE, Saubolle MA, et al. Effectiveness of practices to increase timeliness of providing targeted therapy for inpatients with bloodstream infections: a laboratory medicine best practices systematic review and meta-analysis. Clinical Microbiology Reviews 2015;29(1):59-103. - PMC - PubMed
Deku 2019
-
- Deku JG, Dakorah MP, Lokpo SY, Orish VN, Ussher FA, Kpene GE, et al. The epidemiology of bloodstream infections and antimicrobial susceptibility patterns: a nine-year retrospective study at St. Dominic Hospital, Akwatia, Ghana. Journal of Tropical Medicine 2019;6750864:10. [DOI: 10.1155/2019/6750864] - DOI - PMC - PubMed
Doern 2018
Dyar 2017
-
- Dyar OJ, Huttner B, Schouten J, Pulcini C. What is antimicrobial stewardship? Clinical Microbiology and Infection 2017;23(11):793-8. - PubMed
Ehren 2020
-
- Ehren K, Meibner A, Jazmati N, Wille J, Jung N, Vehreschild JJ, et al. Clinical Impact of rapid species identification from positive blood cultures with same-day phenotypic antimicrobial susceptibility testing on the management and outcome of bloodstream infections. Clinical Infectious Diseases 2020;70(7):1285-93. [DOI: 10.1093/cid/ciz406] - DOI - PubMed
Ferrer 2014
-
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Critical Care Medicine 2014;42(8):1749-55. - PubMed
Goto 2013
-
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clinical Microbiology and Infection 2013;19(6):501-9. - PubMed
GRADE 2014
-
- Puhan MA, Schünemann HJ, Murad MH, Li T, Brignardello-Petersen R, Singh JA, et al. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014;349:g5360. - PubMed
GRADEpro GDT [Computer program]
-
- McMaster University (developed by Evidence Prime) GRADEpro GDT. Version accessed prior to 1 February 2021. Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Guyatt 2011
-
- Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. Journal of Clinical Epidemiology 2011;64(4):380-2. - PubMed
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Huang 2013
-
- Huang A, Newton D, Kunapuli A, Gandhi TN, Washer LL, Isip J, et al. Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia.. Clinical Infectious Diseases 2013;57:1237-45. [DOI: 10.1093/cid/cit498] - DOI - PubMed
Kumar 2006
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Critical Care Medicine 2006;34(6):1589-96. - PubMed
Kumar 2009
-
- Kumar A, Ellis P, Arabi Y, Roberts D, Light B, Parrillo JE, et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 2009;136(5):1237-48. - PubMed
Laupland 2014
Ly 2008
Maurer 2017
Moher 2009
Nicolsen 2013
-
- Nicolsen NC, LeCroy N, Alby K, Martin KE, Laux J, Lin FC, et al. Clinical outcomes with rapid detection of methicillin-resistant and methicillin-susceptible Staphylococcus aureus isolates from routine blood cultures. Journal of Clinical Microbiology 2013;51(12):4126-9. [DOI: 10.1128/JCM.01667-13] - DOI - PMC - PubMed
Pardo 2015
-
- Pardo J, Klinker KP, Borgert SJ, Butler BM, Giglio PG, Rand KH. Clinical and economic impact of antimicrobial stewardship interventions with the FilmArray blood culture identification panel. Diagnostic Microbiology and Infectious Disease 2016;84:159-64. - PubMed
Paul 2010
PHE 2014
-
- Public Health England. Investigation of blood cultures (for organisms other than Mycobacterium species). UK Standards for Microbiology Investigations. B 37 Issue 8. 2014. www.gov.uk/uk-standards-for-microbiology-investigations-smi-qualityand-c... (accessed 1 June 2018).
Popay 2006
-
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews: a product from the ESRC Methods Programme. www.lancs.ac.uk/shm/research/nssr/research/dissemination/publications/NS... (accessed 1 June 2018).
Reddy 2010
Reimer 1997
Review Manager 2020 [Computer program]
-
- The Cochrane Collaboration Review Manager 5 (RevMan 5). Version 5.4. The Cochrane Collaboration, 2020.
Rhodes 2017
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: International guidelines for Management of sepsis and septic shock: 2016. Intensive Care Medicine 2017;43(3):304-77. - PubMed
Silva 2013
Timbrook 2017
Vardakas 2015
-
- Vardakas K, Anifantaki F, Trigkidis KK, Falagas ME. Rapid molecular diagnostic tests in patients with bacteremia: evaluation of their impact on decision making and clinical outcomes. European Journal of Clinical Microbiology & Infectious Diseases 2015;34(11):2149-60. [DOI: 10.1007/s10096-015-2466-y] - DOI - PubMed
Verroken 2016
-
- Verroken A, Defourny L, Waroux OP, Belkhir L, Laterre PF, Delmée M, et al. Correction: clinical impact of MALDI-TOF MS identification and rapid susceptibility testing on adequate antimicrobial treatment in sepsis with positive blood cultures. PloS One 2016;11(9):e0160537. [DOI: 10.1371/journal.pone.0156299] - DOI - PMC - PubMed
WHO 2017
-
- World Health Organization. WHO Secretariat Report A70/13 - Improving the prevention, diagnosis and clinical management of sepsis. www.who.int/servicedeliverysafety/areas/sepsis/en/ (accessed 1 June 2018).
References to other published versions of this review
Anton‐Vazquez 2018
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical