

Learning from the past: Taiwan's responses to COVID-19 versus SARS
- PMID: 34098099
- PMCID: PMC8178059
- DOI: 10.1016/j.ijid.2021.06.002
Learning from the past: Taiwan's responses to COVID-19 versus SARS
Abstract
Objectives: To evaluate the prevalence of infection prevention behaviors in Taiwan-wearing facemasks and alcohol-based hand hygiene (AHH)-and compare their practice rates during SARS and COVID-19.
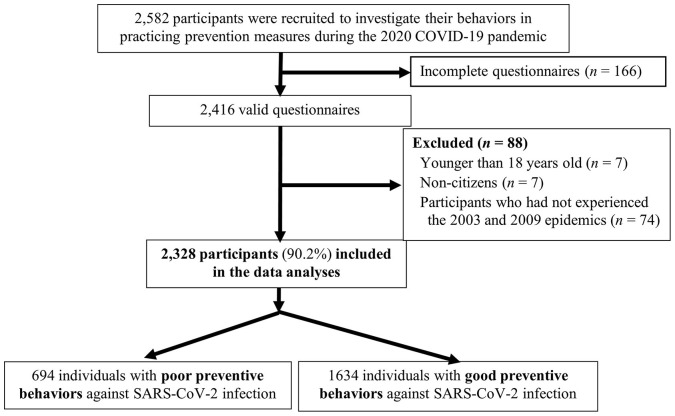
Methods: We surveyed 2328 Taiwanese from July 29 to August 6, 2020, assessing demographics, information sources, and preventive behaviors during the 2003 SARS outbreaks, 2009 pandemic influenza H1N1, COVID-19, and with post-survey intentions. Characteristics associated with the practice of preventive behaviors in 2020 were identified through logistic regression.
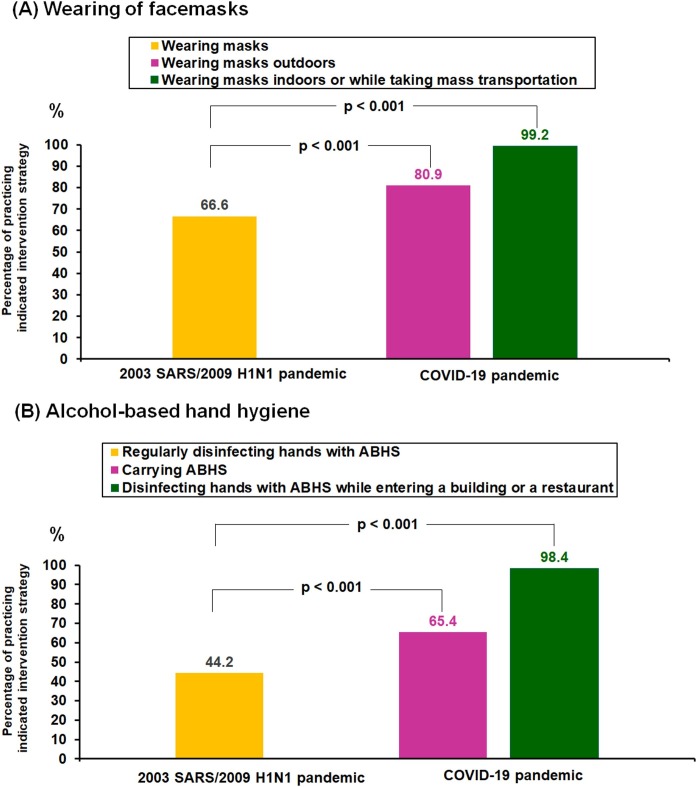
Results: Preventive behaviors were conscientiously practiced by 70.2% of participants. Compared with 2003 SARS/2009 H1N1, the percentages of facemask use (66.6% vs 99.2% [indoors], P < 0.001) and on-person AHH (44.2% vs 65.4% [hand sanitizers], P < 0.001) significantly increasedduring 2020 COVID-19. Highest adherence to preventive behaviors in 2020 was among females (adjusted odds ratio [aOR], 1.72), those receiving government COVID-19 information (aOR, 1.52), participants recruited from primary-care clinics (aOR, 1.43), and those who practiced AHH during 2003 SARS/2009 H1N1 (aOR, 1.37).
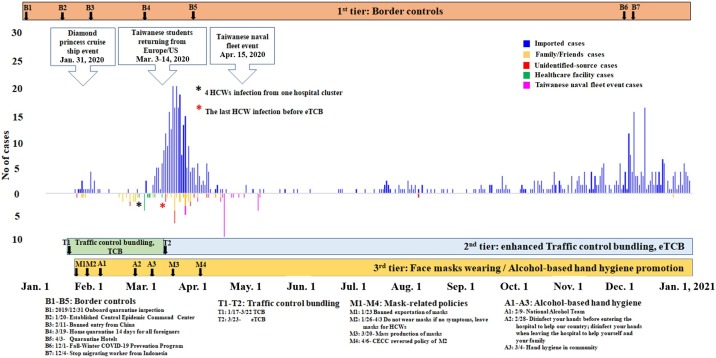
Conclusions: Government leadership, healthcare providers risk communication, and public cooperation rapidly mitigated the spread of COVID-19 in Taiwan even before vaccination. Future global efforts must implement such population-based preventive behaviors at a level above the viral-transmission-threshold, particularly in areas with fast-spreading SARS-CoV-2 variants.
Keywords: Alcohol-based hand hygiene; COVID-19; Face mask; Public health policies; SARS-CoV-2; Taiwan; Threshold-based bundle strategy.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Bundgaard H., Bundgaard J.S., Raaschou-Pedersen D.E.T., Mariager A.F., Schytte N., von Buchwald C., et al. Face masks for the prevention of COVID-19 — rationale and design of the randomised controlled trial DANMASK-19. Dan Med J. 2020;67(9) - PubMed
-
- Buss L.F., Prete C.A., Jr, Abrahim C.M.M., Mendrone A., Jr, Salomon T., de Almeida-Neto C., et al. Three-quarters attack rate of SARS-CoV-2 in the Brazilian Amazon during a largely unmitigated epidemic. Science. 2021;371(6526):288–292. doi: 10.1126/science.abe9728. PMID: 33293339; PMCID: PMC7857406. - DOI - PMC - PubMed
-
- Chen P.C., Lin H.H., Chang S.S., Lu T.P., Chang H.H. Health behavior monitoring of new life movement for COVID-19 disease prevention. 2020 Annual Conference of Taiwan Public Health Association on October 17, 2020 in Taipei, Taiwan. 2020
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
