

Demographic, Clinical, and Psychosocial Predictors of Change in Medication Adherence in the Support, Educate, Empower Program
- PMID: 34098169
- PMCID: PMC8716681
- DOI: 10.1016/j.ogla.2021.06.001
Demographic, Clinical, and Psychosocial Predictors of Change in Medication Adherence in the Support, Educate, Empower Program
Abstract
Purpose: To investigate whether demographic, clinical, or psychosocial factors act as moderators of change in medication adherence in the Support, Educate, Empower (SEE) program.
Design: Prospective, single-arm pilot study with a pre-post design.
Participants: Patients with glaucoma aged ≥ 40 years and taking ≥ 1 glaucoma medication were recruited from the University of Michigan Kellogg Eye Center. Those who had electronically measured adherence ≤ 80% in the 3-month eligibility monitoring period were enrolled in the SEE program.
Methods: Medication adherence was monitored electronically during the 7-month intervention and calculated as the percentage of doses taken correctly. Change in adherence at different points in the SEE program and cumulative change in adherence were modeled with linear regression, and baseline demographic, clinical, and psychosocial factors were investigated for significant associations.
Main outcome measures: Demographic, clinical, and psychosocial variables associated with change in medication adherence in the SEE program.
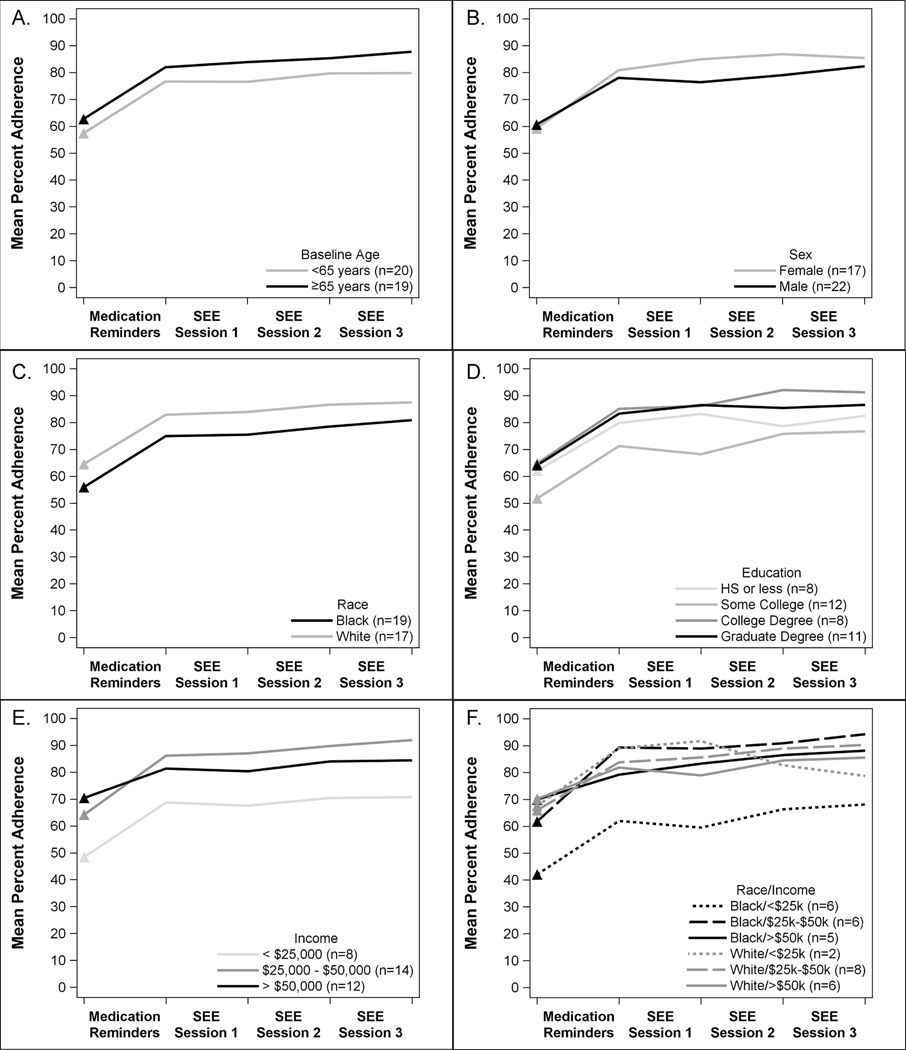
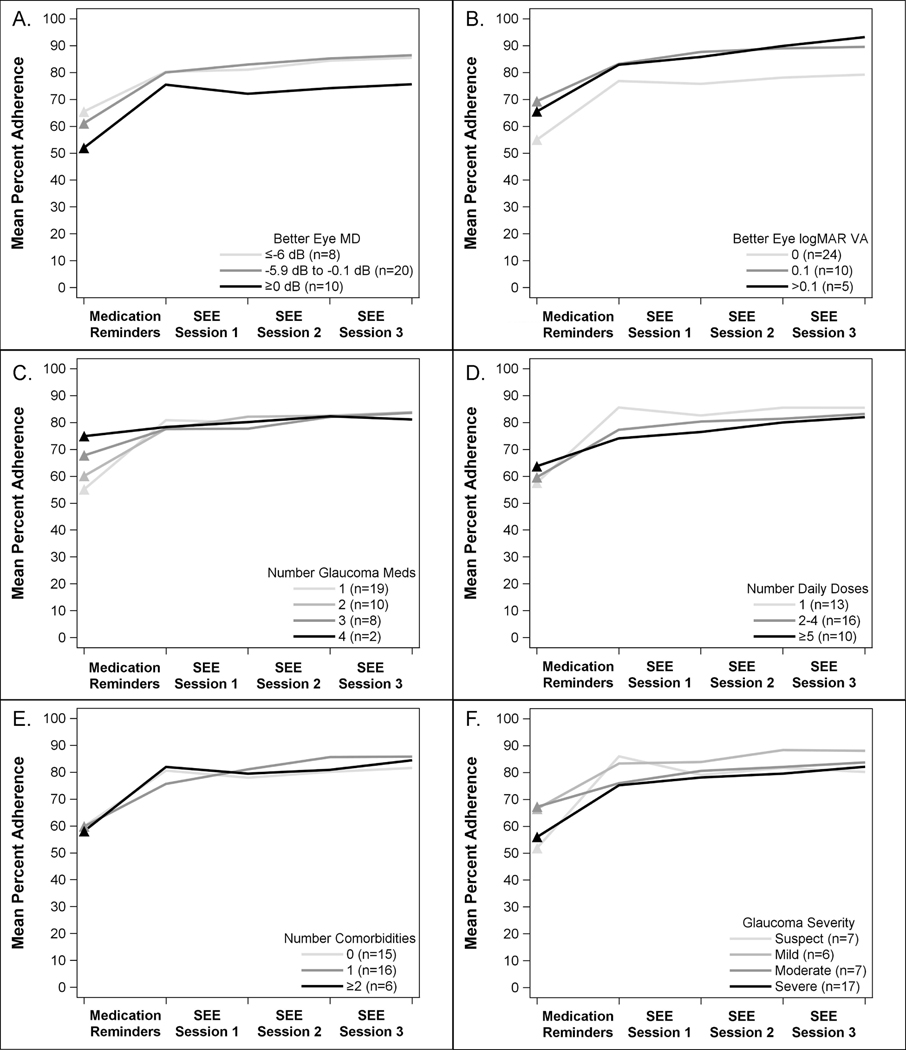
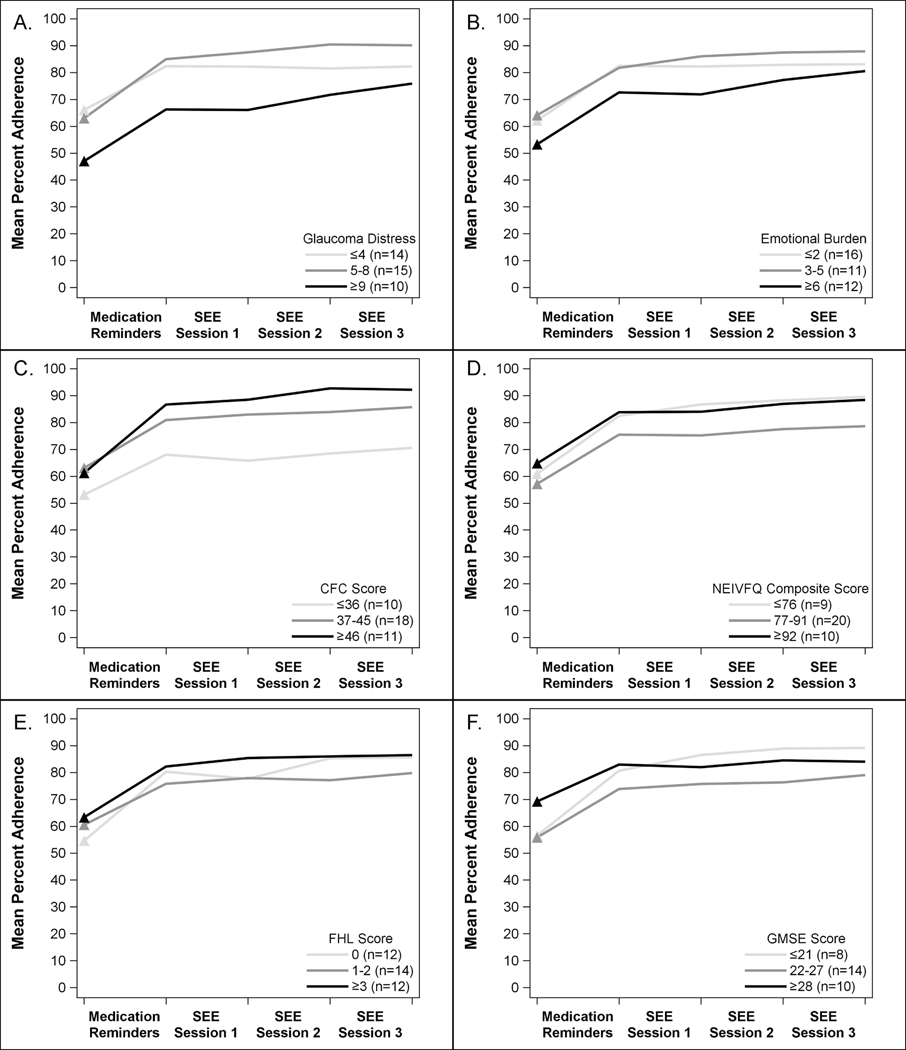
Results: Thirty-nine participants completed the SEE program. These participants were on average 63.9 years old (standard deviation [SD], 10.7 years), 56% (n = 22) were male, 44% (n = 17) were White, and 49% (n = 19) were Black. Medication adherence improved from an average of 59.9% (SD, 18.5%) at baseline to 83.6% (SD, 17.5%) after the final SEE session, for an increase of 23.7% (SD, 17.5%). Although participants with lower income (< $25 000 and $25 000-50 000 vs. >$50 000) had lower baseline adherence (48.4% and 64.1% vs. 70.4%), these individuals had greater increases in adherence during the first month of medication reminders (19.6% and 21.6% vs. 10.2%; P = 0.05 and P = 0.007, respectively). Participants taking fewer glaucoma medications also had significantly greater increases in adherence with medication reminders (P < 0.001). Those with higher levels of glaucoma-related distress (GD) had lower baseline adherence and greater increases in adherence with glaucoma coaching (P = 0.06).
Conclusions: Patient-level factors associated with relatively greater improvements in medication adherence through the SEE Program included lower income, fewer glaucoma medications, and increased GD. These findings demonstrate that the SEE program can improve glaucoma self-management even among participants with social and psychological barriers to medication adherence.
Keywords: Counseling; Glaucoma; Medication adherence; Medication reminders; Motivational interviewing; Personalized education; Support.
Copyright © 2021 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Glaucoma Medication Adherence 1 Year after the Support, Educate, Empower Personalized Glaucoma Coaching Program.Ophthalmol Glaucoma. 2023 Jan-Feb;6(1):23-28. doi: 10.1016/j.ogla.2022.08.001. Epub 2022 Aug 8. Ophthalmol Glaucoma. 2023. PMID: 35953021 Free PMC article.
-
The Impact of the Support, Educate, Empower Personalized Glaucoma Coaching Pilot Study on Glaucoma Medication Adherence.Ophthalmol Glaucoma. 2020 Jul-Aug;3(4):228-237. doi: 10.1016/j.ogla.2020.04.013. Epub 2020 Apr 30. Ophthalmol Glaucoma. 2020. PMID: 33012330 Free PMC article.
-
Psychosocial Predictors of Glaucoma Medication Adherence Among the Support, Educate, Empower (SEE) Personalized Glaucoma Coaching Pilot Study Participants.Am J Ophthalmol. 2020 Aug;216:207-218. doi: 10.1016/j.ajo.2020.02.009. Epub 2020 Feb 19. Am J Ophthalmol. 2020. PMID: 32087145 Free PMC article.
-
Review of glaucoma medication adherence monitoring in the digital health era.Br J Ophthalmol. 2023 Feb;107(2):153-159. doi: 10.1136/bjophthalmol-2020-317918. Epub 2021 Apr 15. Br J Ophthalmol. 2023. PMID: 33858837 Free PMC article. Review.
-
Adherence and factors influencing adherence to glaucoma medications among adult glaucoma patients in Ethiopia: A systematic review and meta-analysis.PLoS One. 2024 Mar 13;19(3):e0293047. doi: 10.1371/journal.pone.0293047. eCollection 2024. PLoS One. 2024. PMID: 38478513 Free PMC article.
Cited by
-
Patient-Centered Outcomes After a Medication Adherence Intervention: a Pilot Study.J Glaucoma. 2023 Oct 1;32(10):891-899. doi: 10.1097/IJG.0000000000002228. Epub 2023 Mar 30. J Glaucoma. 2023. PMID: 37054438 Free PMC article.
-
Socioeconomic Disparities in Glaucoma Severity at Initial Diagnosis: A Nationwide Electronic Health Record Cohort Analysis.Am J Ophthalmol. 2024 Jul;263:50-60. doi: 10.1016/j.ajo.2024.02.022. Epub 2024 Feb 22. Am J Ophthalmol. 2024. PMID: 38395325 Free PMC article.
-
Factors Affecting Glaucoma Medication Adherence and Interventions to Improve Adherence: A Narrative Review.Ophthalmol Ther. 2023 Dec;12(6):2863-2880. doi: 10.1007/s40123-023-00797-8. Epub 2023 Sep 12. Ophthalmol Ther. 2023. PMID: 37698824 Free PMC article. Review.
-
Glaucoma Medication Adherence 1 Year after the Support, Educate, Empower Personalized Glaucoma Coaching Program.Ophthalmol Glaucoma. 2023 Jan-Feb;6(1):23-28. doi: 10.1016/j.ogla.2022.08.001. Epub 2022 Aug 8. Ophthalmol Glaucoma. 2023. PMID: 35953021 Free PMC article.
-
Tools to measure barriers to medication management capacity in older adults: a scoping review.BMC Geriatr. 2024 Mar 27;24(1):285. doi: 10.1186/s12877-024-04893-7. BMC Geriatr. 2024. PMID: 38532328 Free PMC article.
References
-
- Bourne RRA, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. The Lancet Global Health. 2013;1(6):e339–e349. - PubMed
-
- Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. - PubMed
-
- Nordstrom BL, Friedman DS, Mozaffari E, Quigley HA, Walker AM. Persistence and Adherence With Topical Glaucoma Therapy. Am J Ophthalmol. 2005;140(4):598.e591–598.e511. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
