

Re-exploration for bleeding after cardiac surgery: revaluation of urgency and factors promoting low rate
- PMID: 34099003
- PMCID: PMC8183590
- DOI: 10.1186/s13019-021-01545-4
Re-exploration for bleeding after cardiac surgery: revaluation of urgency and factors promoting low rate
Abstract
Background: Re-exploration of bleeding after cardiac surgery is associated with significant morbidity and mortality. Perioperative blood loss and rate of re-exploration are variable among centers and surgeons.
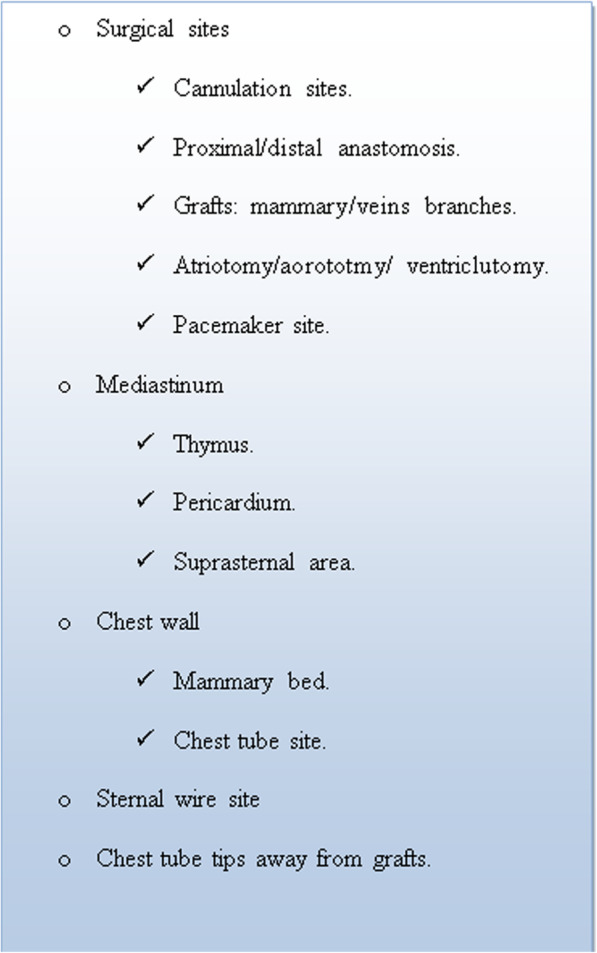
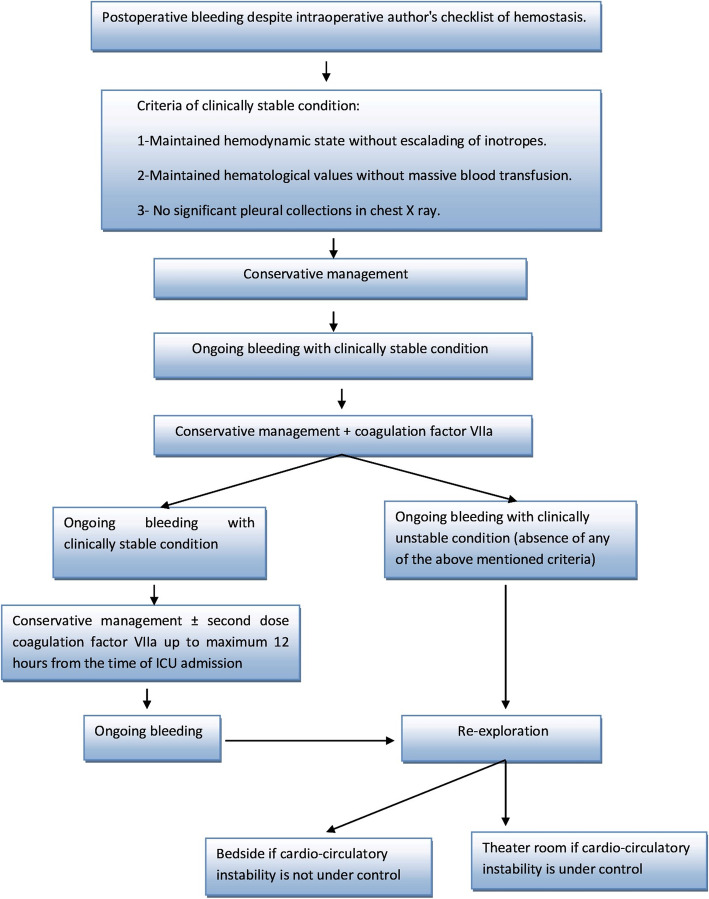
Objective: To present our experience of low rate of re-exploration based on adopting checklist for hemostasis and algorithm for management.
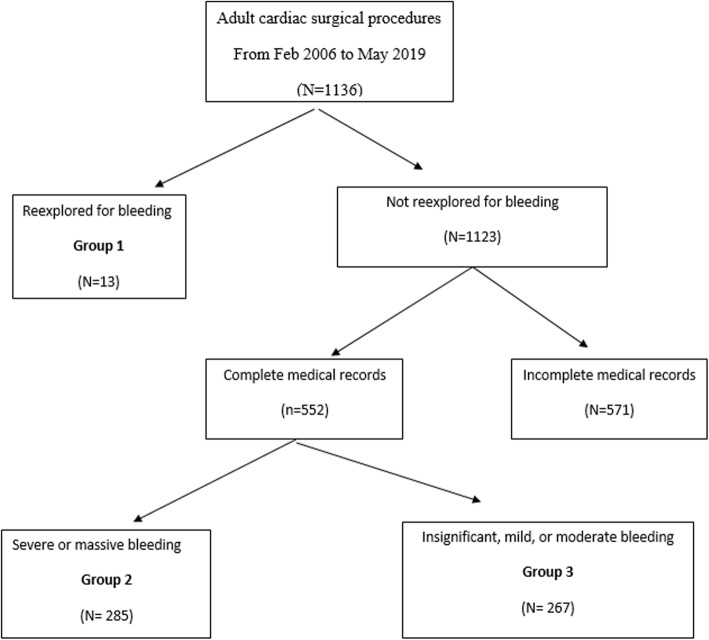
Methods: Retrospective analysis of medical records was conducted for 565 adult patients who underwent surgical treatment of congenital and acquired heart disease and were complicated by postoperative bleeding from Feb 2006 to May 2019. Demographics of patients, operative characteristics, perioperative risk factors, blood loss, requirements of blood transfusion, morbidity and mortality were recorded. Logistic regression was used to identify predictors of re-exploration and determinants of adverse outcome.
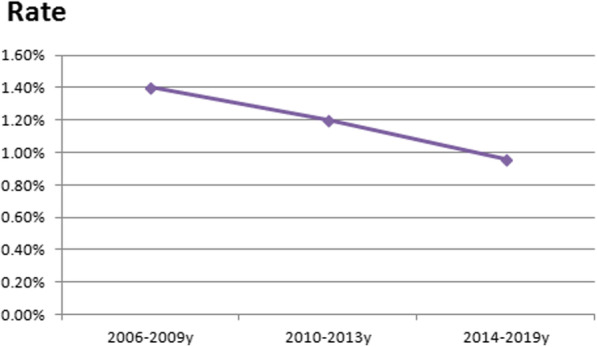
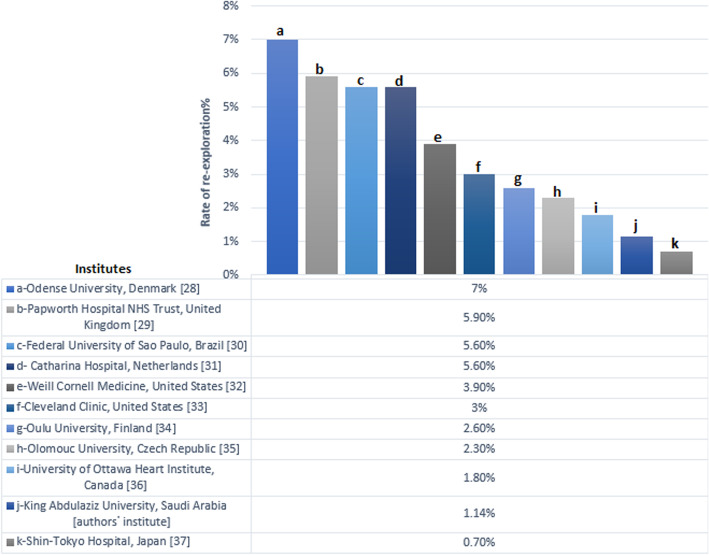
Results: Thirteen patients (1.14%) were reexplored for bleeding. An identifiable source of bleeding was found in 11 (84.6%) patients. Risk factors for re-exploration were high body mass index, high Euro SCORE, operative priority (urgent/emergent), elevated serum creatinine and low platelets count. Re-exploration was significantly associated with increased requirements of blood transfusion, adverse effects on cardiorespiratory state (low ejection fraction, increased s. lactate, and prolonged period of mechanical ventilation), longer intensive care unit stay, hospital stay, increased incidence of SWI, and higher mortality (15.4% versus 2.53% for non-reexplored patients). We managed 285 patients with severe or massive bleeding conservatively by hemostatic agents according to our protocol with no added risk of morbidity or mortality.
Conclusion: Low rate of re-exploration for bleeding can be achieved by strict preoperative preparation, intraoperative checklist for hemostasis implemented by senior surgeons and adopting an algorithm for management.
Keywords: Bleeding; Cardiac surgery; Re-exploration.
Conflict of interest statement
All authors declare that they have no competing interests.
Figures
References
-
- Murphy GJ, Pike K, Rogers CA, Wordsworth S, Stokes EA, Angelini GD, et al. Liberal or restrictive transfusion after cardiac surgery. N Engl J Med. 2015;372(11):997–1008. 10.1056/NEJMoa1403612. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
