

Implementation of peer specialist services in VA primary care: a cluster randomized trial on the impact of external facilitation
- PMID: 34099004
- PMCID: PMC8183089
- DOI: 10.1186/s13012-021-01130-2
Implementation of peer specialist services in VA primary care: a cluster randomized trial on the impact of external facilitation
Abstract
Background: Over 1100 veterans work in the Veterans Health Administration (VHA) as peer specialists (PSs)-those with formal training who support other veterans with similar diagnoses. A White House Executive Action mandated the pilot reassignment of VHA PSs from their usual placement in mental health to 25 primary care Patient Aligned Care Teams (PACTs) in order to broaden the provision of wellness services that can address many chronic illnesses. An evaluation of this initiative was undertaken to assess the impact of outside assistance on the deployment of PSs in PACTs, as implementation support is often needed to prevent challenges commonly experienced when first deploying PSs in new settings.
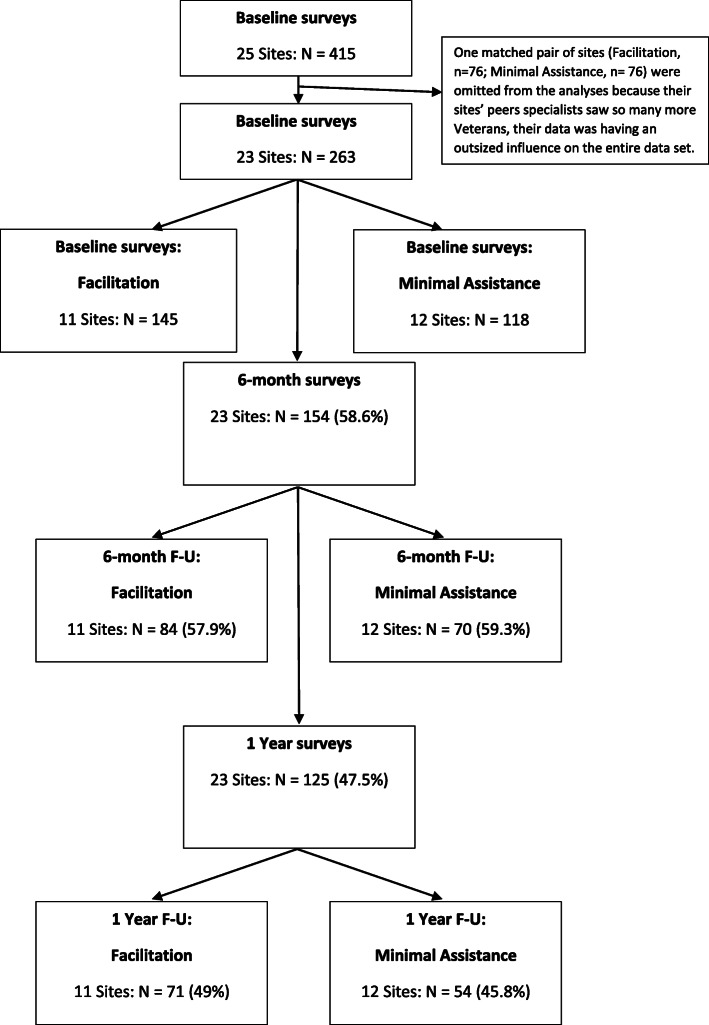
Methods: This study was a cluster-randomized hybrid II effectiveness-implementation trial to test the impact of minimal implementation support vs. facilitated implementation on the deployment of VHA PSs in PACT over 2 years. Twenty-five Veterans Affairs Medical Centers (VAMCs) were recruited to reassign mental health PSs to provide wellness-oriented care in PACT. Sites in three successive cohorts (n = 7, 10, 8) over 6-month blocks were matched and randomized to each study condition. In facilitated implementation, an outside expert worked with site stakeholders through a site visit and regular calls, and provided performance data to guide the planning and address challenges. Minimal implementation sites received a webinar and access to the VHA Office of Mental Health Services work group. The two conditions were compared on PS workload data and veteran measures of activation, satisfaction, and functioning. Qualitative interviews collected information on perceived usefulness of the PS services.
Results: In the first year, sites that received facilitation had higher numbers of unique veterans served and a higher number of PS visits, although the groups did not differ after the second year. Also, sites receiving external facilitation started delivering PS services more quickly than minimal support sites. All sites in the external facilitation condition continued in the pilot into the second year, whereas two of the sites in the minimal assistance condition dropped out after the first year. There were no differences between groups on veterans' outcomes-activation, satisfaction, and functioning. Most veterans were very positive about the help they received as evidenced in the qualitative interviews.
Discussion: These findings demonstrate that external facilitation can be effective in supporting the implementation of PSs in primary care settings. The lack of significant differences across conditions after the second year highlights the positive outcomes associated with active facilitation, while also raising the important question of whether longer-term success may require some level of ongoing facilitation and implementation support.
Trial registration: This project is registered at ClinicalTrials.gov with number NCT02732600 (URL: https://clinicaltrials.gov/ct2/show/NCT02732600 ).
Keywords: Facilitation; Implementation; Peer specialist; Primary care.
Conflict of interest statement
The authors declare that they have no competing interests.
Similar articles
-
Barriers and Enablers to Implementing Peer Specialists in Veterans Health Administration Primary Care: a Qualitative Study.J Gen Intern Med. 2023 Feb;38(3):707-714. doi: 10.1007/s11606-022-07782-0. Epub 2022 Sep 20. J Gen Intern Med. 2023. PMID: 36127539 Free PMC article.
-
Provision of peer specialist services in VA patient aligned care teams: protocol for testing a cluster randomized implementation trial.Implement Sci. 2017 May 2;12(1):57. doi: 10.1186/s13012-017-0587-7. Implement Sci. 2017. PMID: 28464935 Free PMC article. Clinical Trial.
-
A two-state comparative implementation of peer-support intervention to link veterans to health-related services after incarceration: a study protocol.BMC Health Serv Res. 2017 Sep 12;17(1):647. doi: 10.1186/s12913-017-2572-x. BMC Health Serv Res. 2017. PMID: 28899394 Free PMC article.
-
Peer specialist-led interventions in primary care at the Veterans Health Administration: An integrative review.Psychol Serv. 2025 May;22(2):256-269. doi: 10.1037/ser0000858. Epub 2024 Apr 11. Psychol Serv. 2025. PMID: 38602826 Review.
-
Delivery of gender-sensitive comprehensive primary care to women veterans: implications for VA Patient Aligned Care Teams.J Gen Intern Med. 2014 Jul;29 Suppl 2(Suppl 2):S703-7. doi: 10.1007/s11606-013-2699-3. J Gen Intern Med. 2014. PMID: 24715395 Free PMC article. Review.
Cited by
-
Cluster-randomized implementation trial of two facilitation strategies to implement a novel information and communications technology at the Veterans Health Administration.Implement Sci. 2024 Jan 2;19(1):1. doi: 10.1186/s13012-023-01329-5. Implement Sci. 2024. PMID: 38166974 Free PMC article.
-
Barriers and Enablers to Implementing Peer Specialists in Veterans Health Administration Primary Care: a Qualitative Study.J Gen Intern Med. 2023 Feb;38(3):707-714. doi: 10.1007/s11606-022-07782-0. Epub 2022 Sep 20. J Gen Intern Med. 2023. PMID: 36127539 Free PMC article.
-
Impact of Implementation Facilitation on the REACH VET Clinical Program for Veterans at Risk for Suicide.Psychiatr Serv. 2024 Aug 1;75(8):726-732. doi: 10.1176/appi.ps.20230277. Epub 2024 Mar 6. Psychiatr Serv. 2024. PMID: 38444365 Free PMC article.
-
Supporting servicemembers and veterans during their transition to civilian life using certified sponsors: A three-arm randomized controlled trial.Psychol Serv. 2023;20(Suppl 2):248-259. doi: 10.1037/ser0000764. Epub 2023 Jun 29. Psychol Serv. 2023. PMID: 37384439 Free PMC article. Clinical Trial.
-
"It's more than a ride" veteran perceptions of peer specialist qualities and activities that were most valuable for post-incarceration reentry: a qualitative analysis.Health Justice. 2025 Jan 10;13(1):2. doi: 10.1186/s40352-024-00303-7. Health Justice. 2025. PMID: 39792224 Free PMC article.
References
-
- Rosland AM, Nelson K, Sun H, Dolan ED, Maynard C, Bryson C, et al. The patient-centered medical home in the Veterans Health Administration. Am J ManagCare. 2013;19(7):e263–ee72. - PubMed
-
- Lim LL, Lau ESH, Kong APS, Davies MJ, Levitt NS, Eliasson B, Aguilar-Salinas CA, Ning G, Seino Y, So WY, McGill M, Ogle GD, Orchard TJ, Clarke P, Holman RR, Gregg EW, Gagliardino JJ, Chan JCN. Aspects of multicomponent integrated care promote sustained improvement in surrogate clinical outcomes: a systematic review and meta-analysis. Diabetes Care. 2018;41(6):1312–1320. doi: 10.2337/dc17-2010. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
