

Staphylococcus aureus ventilator-associated pneumonia in patients with COVID-19: clinical features and potential inference with lung dysbiosis
- PMID: 34099016
- PMCID: PMC8182737
- DOI: 10.1186/s13054-021-03623-4
Staphylococcus aureus ventilator-associated pneumonia in patients with COVID-19: clinical features and potential inference with lung dysbiosis
Abstract
Background: Hospitalized patients with COVID-19 admitted to the intensive care unit (ICU) and requiring mechanical ventilation are at risk of ventilator-associated bacterial infections secondary to SARS-CoV-2 infection. Our study aimed to investigate clinical features of Staphylococcus aureus ventilator-associated pneumonia (SA-VAP) and, if bronchoalveolar lavage samples were available, lung bacterial community features in ICU patients with or without COVID-19.
Methods: We prospectively included hospitalized patients with COVID-19 across two medical ICUs of the Fondazione Policlinico Universitario A. Gemelli IRCCS (Rome, Italy), who developed SA-VAP between 20 March 2020 and 30 October 2020 (thereafter referred to as cases). After 1:2 matching based on the simplified acute physiology score II (SAPS II) and the sequential organ failure assessment (SOFA) score, cases were compared with SA-VAP patients without COVID-19 (controls). Clinical, microbiological, and lung microbiota data were analyzed.
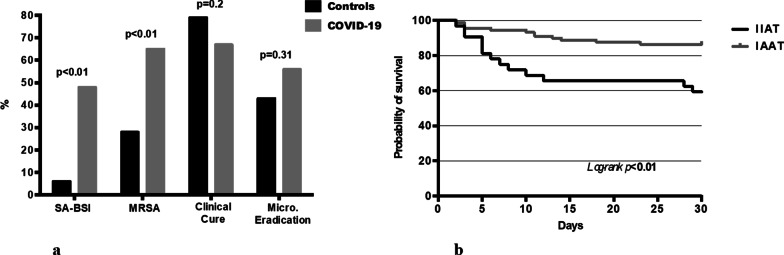
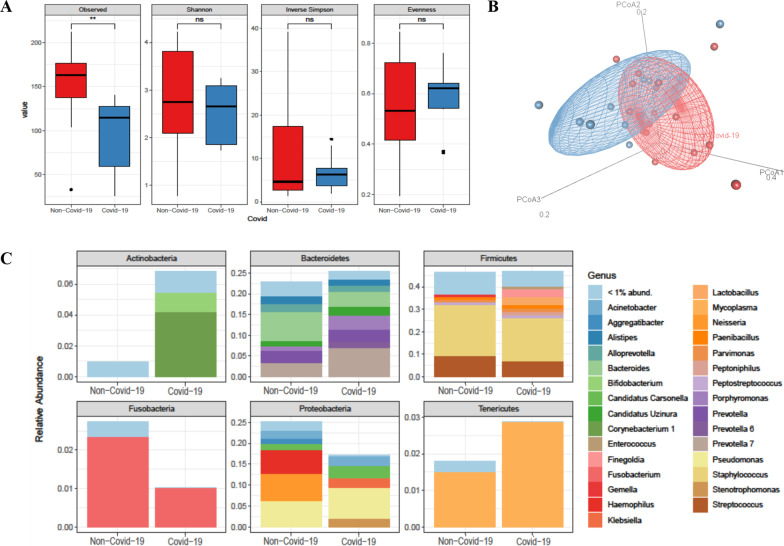
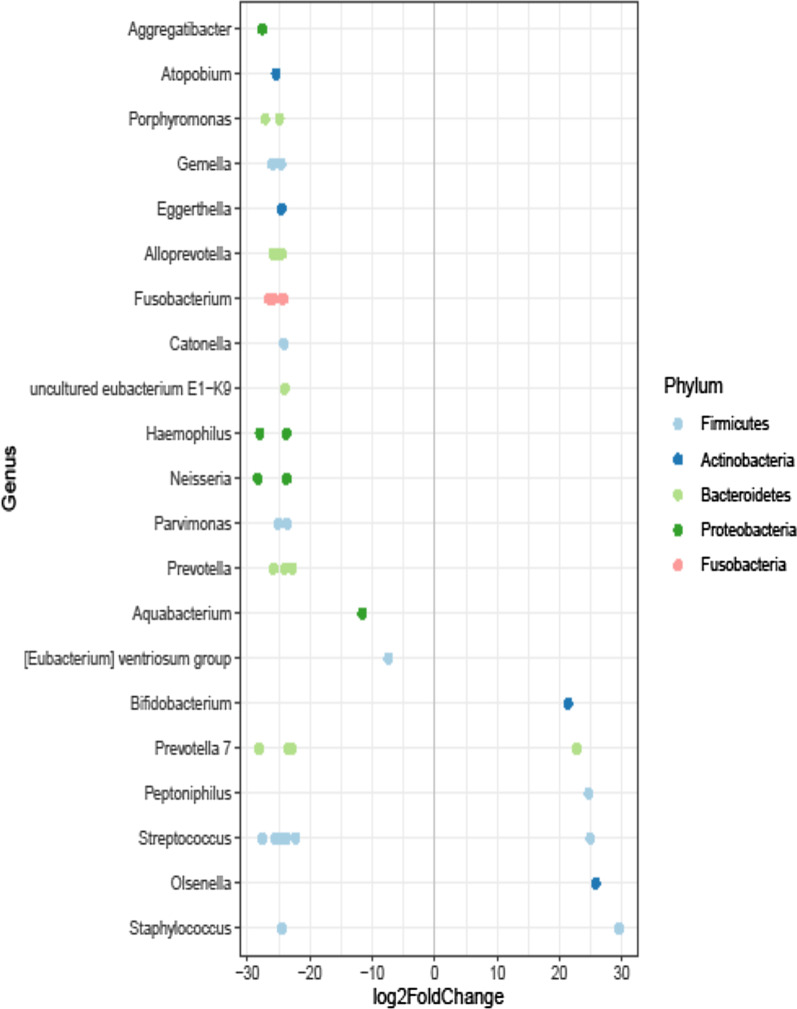
Results: We studied two groups of patients (40 COVID-19 and 80 non-COVID-19). COVID-19 patients had a higher rate of late-onset (87.5% versus 63.8%; p = 0.01), methicillin-resistant (65.0% vs 27.5%; p < 0.01) or bacteremic (47.5% vs 6.3%; p < 0.01) infections compared with non-COVID-19 patients. No statistically significant differences between the patient groups were observed in ICU mortality (p = 0.12), clinical cure (p = 0.20) and microbiological eradication (p = 0.31). On multivariable logistic regression analysis, SAPS II and initial inappropriate antimicrobial therapy were independently associated with ICU mortality. Then, lung microbiota characterization in 10 COVID-19 and 16 non-COVID-19 patients revealed that the overall microbial community composition was significantly different between the patient groups (unweighted UniFrac distance, R2 0.15349; p < 0.01). Species diversity was lower in COVID-19 than in non COVID-19 patients (94.4 ± 44.9 vs 152.5 ± 41.8; p < 0.01). Interestingly, we found that S. aureus (log2 fold change, 29.5), Streptococcus anginosus subspecies anginosus (log2 fold change, 24.9), and Olsenella (log2 fold change, 25.7) were significantly enriched in the COVID-19 group compared to the non-COVID-19 group of SA-VAP patients.
Conclusions: In our study population, COVID-19 seemed to significantly affect microbiological and clinical features of SA-VAP as well as to be associated with a peculiar lung microbiota composition.
Keywords: Bronchoalveolar lavage; COVID-19; Lung microbiota; Staphylococcus aureus; Ventilator-associated pneumonia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. COVID-19 Weekly Epidemiological Update 22. World Heal Organ. 2021;1–3. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/w...
-
- Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, Escalera-Antezana JP, et al. Clinical, laboratory and imaging features of COVID-19: a systematic review and meta-analysis. Travel Med Infect Dis. 2020;34:101623. doi: 10.1016/j.tmaid.2020.101623. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
