

Postpartum mental illness during the COVID-19 pandemic: a population-based, repeated cross-sectional study
- PMID: 34099467
- PMCID: PMC8203259
- DOI: 10.1503/cmaj.210151
Postpartum mental illness during the COVID-19 pandemic: a population-based, repeated cross-sectional study
Abstract
Background: It is unclear whether the clinical burden of postpartum mental illness has increased during the COVID-19 pandemic. We sought to compare physician visit rates for postpartum mental illness in Ontario, Canada, during the pandemic with rates expected based on prepandemic patterns.
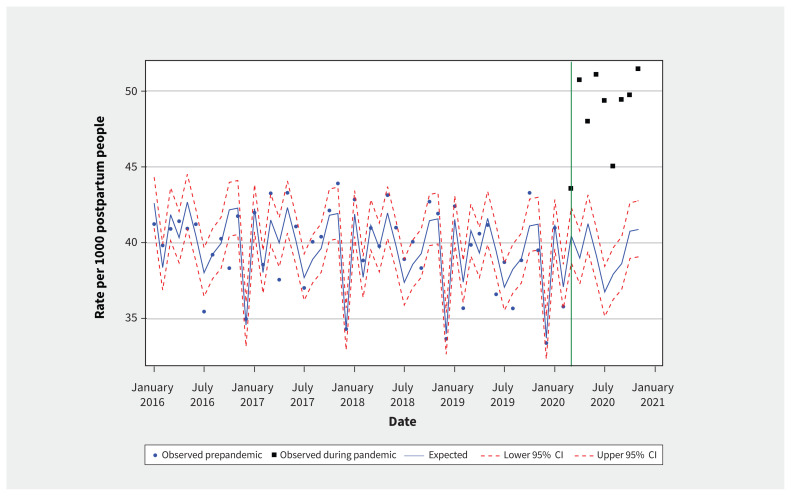
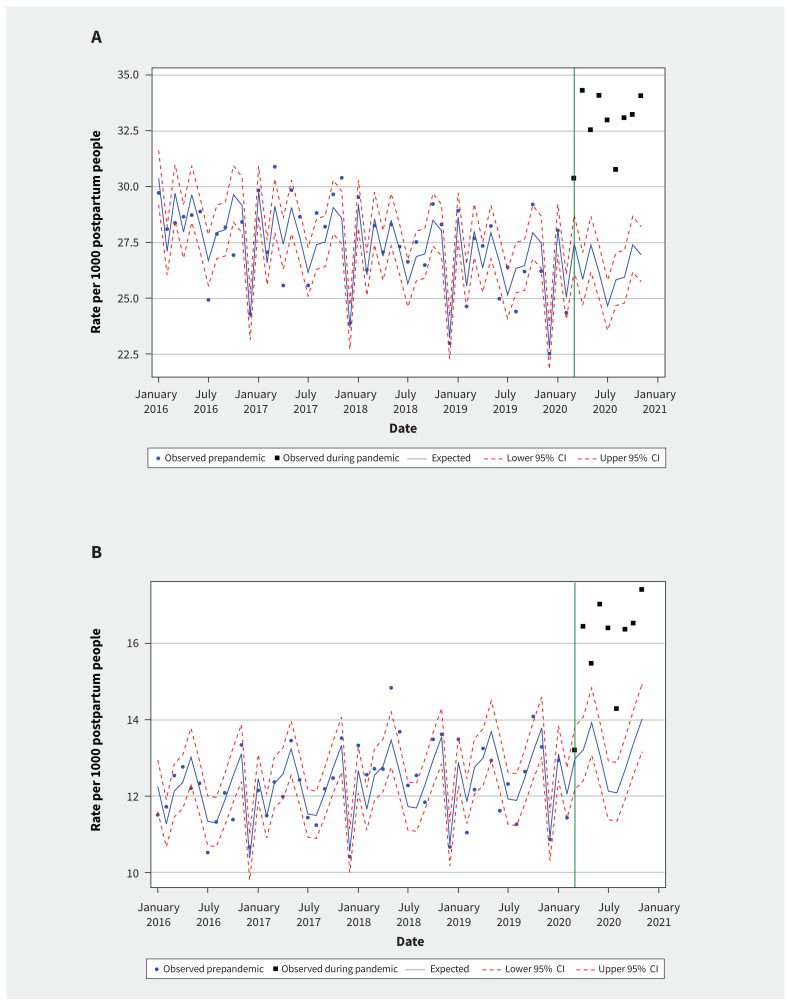
Methods: In this population-based, repeated cross-sectional study using linked health administrative databases in Ontario, Canada, we used negative binomial regression to model expected visit rates per 1000 postpartum people for March-November 2020 based on prepandemic data (January 2016-February 2020). We compared observed visit rates to expected visit rates for each month of the pandemic period, generating absolute rate differences, incidence rate ratios (IRRs) and their 95% confidence intervals (CIs). The primary outcome was a visit to a primary care physician or a psychiatrist for any mental disorder. We stratified analyses by maternal sociodemographic characteristics.
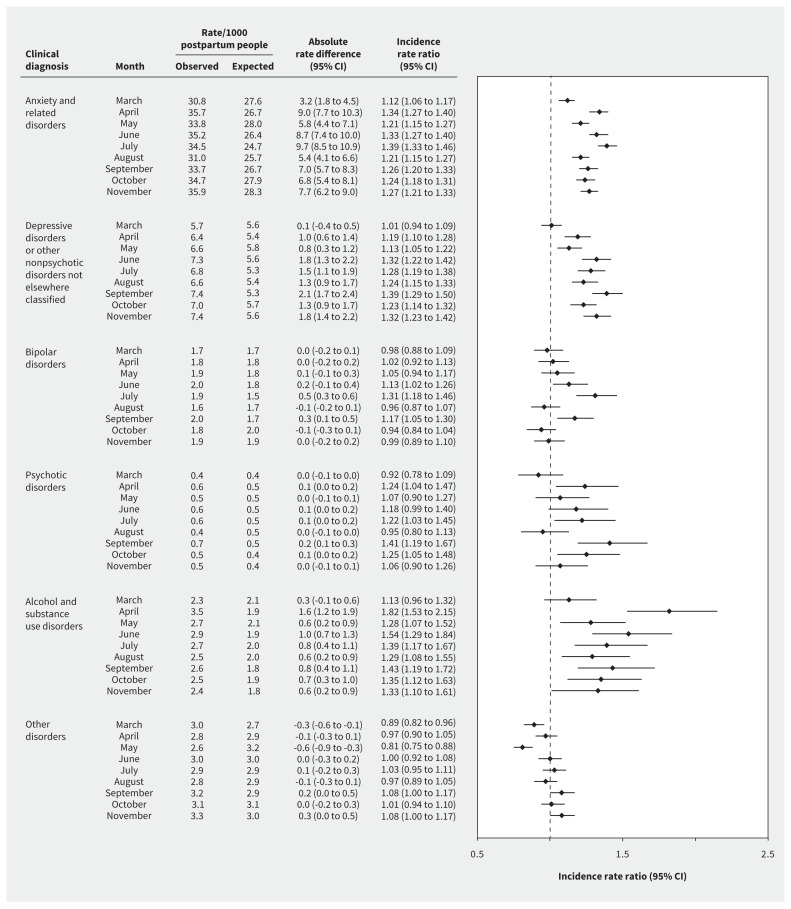
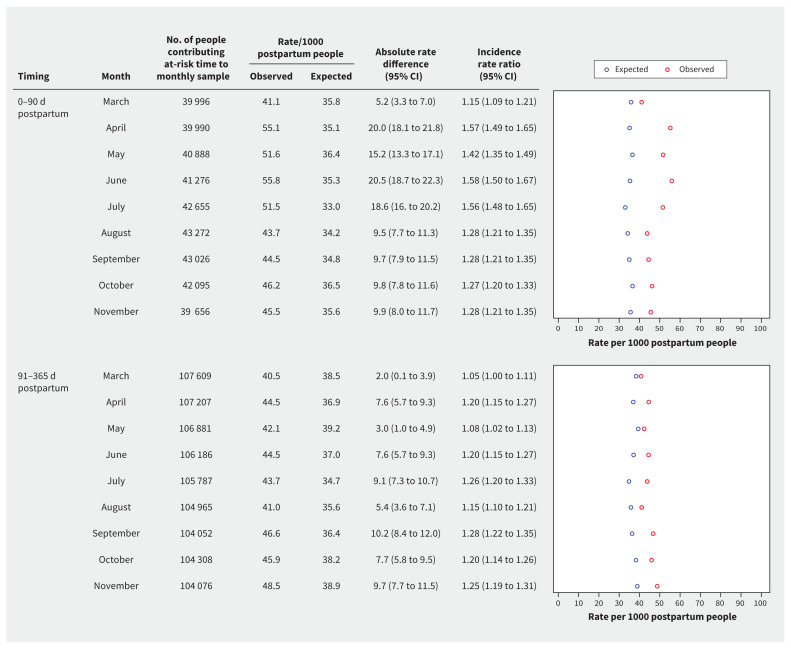
Results: In March 2020, the visit rate was 43.5/1000, with a rate difference of 3.11/1000 (95% CI 1.25-4.89) and an IRR of 1.08 (95% CI 1.03-1.13) compared with the expected rate. In April, the rate difference (10.9/1000, 95% CI 9.14-12.6) and IRR (1.30, 95% CI 1.24-1.36) were higher; this level was generally sustained through November 2020. From April-November, we observed elevated visit rates across provider types and for diagnoses of anxiety, depressive and alcohol or substance use disorders. Observed increases from expected visit rates were greater for people 0-90 days postpartum compared with 91-365 days postpartum; increases were small among people living in low-income neighbourhoods. Public health units in the northern areas of the province did not see sustained elevations in visit rates after July; southern health units had elevated rates through to November.
Interpretation: Increased visits for mental health conditions among postpartum people during the first 9 months of the COVID-19 pandemic suggest an increased need for effective and accessible mental health care for this population as the pandemic progresses.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Simone Vigod and Sophie Grigoriadis report royalties from UpToDate Inc for materials on perinatal depression. Elisabeth Wright reports grants from the Women’s College Hospital Academic and Medical Services Group, and an honorarium for training as a provider for a clinical trial on perinatal psychotherapy. She is also a member of her hospital’s Interim Equity Committee. Sophie Grigoriadis reports royalties from the Canadian Pharmacists Association, Norton, Myriad Neuroscience and Abbie for materials, consultations and presentations related to depression. No other competing interests were declared.
Figures
Similar articles
-
Utilization of Physician-Based Mental Health Care Services Among Children and Adolescents Before and During the COVID-19 Pandemic in Ontario, Canada.JAMA Pediatr. 2022 Apr 1;176(4):e216298. doi: 10.1001/jamapediatrics.2021.6298. Epub 2022 Apr 4. JAMA Pediatr. 2022. PMID: 35129604 Free PMC article.
-
Mental Health Hospitalizations in Canadian Children, Adolescents, and Young Adults Over the COVID-19 Pandemic.JAMA Netw Open. 2024 Jul 1;7(7):e2422833. doi: 10.1001/jamanetworkopen.2024.22833. JAMA Netw Open. 2024. PMID: 38976264 Free PMC article.
-
Physician Health Care Visits for Mental Health and Substance Use During the COVID-19 Pandemic in Ontario, Canada.JAMA Netw Open. 2022 Jan 4;5(1):e2143160. doi: 10.1001/jamanetworkopen.2021.43160. JAMA Netw Open. 2022. PMID: 35061041 Free PMC article.
-
Access and use of general and mental health services before and during the COVID-19 pandemic: a systematic review and meta-analysis.BMJ Open. 2025 Mar 12;15(3):e091342. doi: 10.1136/bmjopen-2024-091342. BMJ Open. 2025. PMID: 40074252 Free PMC article.
-
Mental Health in the Time of the COVID-19 Pandemic: A Scoping Review of Collateral Effects on Common Mental Disorders (CMDs).Int J Environ Res Public Health. 2025 Mar 23;22(4):478. doi: 10.3390/ijerph22040478. Int J Environ Res Public Health. 2025. PMID: 40283707 Free PMC article.
Cited by
-
Sex differences among children, adolescents and young adults for mental health service use within inpatient and outpatient settings, before and during the COVID-19 pandemic: a population-based study in Ontario, Canada.BMJ Open. 2023 Nov 1;13(11):e073616. doi: 10.1136/bmjopen-2023-073616. BMJ Open. 2023. PMID: 37914301 Free PMC article.
-
Women's Preferences and Design Recommendations for a Postpartum Depression Psychoeducation Intervention: User Involvement Study.JMIR Form Res. 2022 Jun 23;6(6):e33411. doi: 10.2196/33411. JMIR Form Res. 2022. PMID: 35737435 Free PMC article.
-
The Impact of Covid-19 on Women's Mental Health and Wellbeing During Pregnancy and the Perinatal Period: A Mixed-Methods Systematic Review.Inquiry. 2024 Jan-Dec;61:469580241301521. doi: 10.1177/00469580241301521. Inquiry. 2024. PMID: 39584572 Free PMC article.
-
Postpartum people's experiences of and responses to the COVID-19 pandemic during the first year of the pandemic: A descriptive qualitative study.Womens Health (Lond). 2023 Jan-Dec;19:17455057231157480. doi: 10.1177/17455057231157480. Womens Health (Lond). 2023. PMID: 36846969 Free PMC article.
-
Temporal trends of suicide-related non-traumatic out-of-hospital cardiac arrest characteristics and outcomes with the COVID-19 pandemic.Resusc Plus. 2022 Mar 3;9:100216. doi: 10.1016/j.resplu.2022.100216. eCollection 2022 Mar. Resusc Plus. 2022. PMID: 35261992 Free PMC article.
References
-
- Vigod SN, Stewart DE. Emergent research in the cause of mental illness in women across the lifespan. Curr Opin Psychiatry 2009;22:396–400. - PubMed
-
- Khalifeh H, Hunt IM, Appleby L, et al. . Suicide in perinatal and non-perinatal women in contact with psychiatric services: 15 year findings from a UK national inquiry. Lancet Psychiatry 2016;3:233–42. - PubMed
-
- Stein A, Pearson RM, Goodman SH, et al. . Effects of perinatal mental disorders on the fetus and child. Lancet 2014;384:1800–19. - PubMed
-
- Woolhouse H, Gartland D, Mensah F, et al. . Maternal depression from early pregnancy to 4 years postpartum in a prospective pregnancy cohort study: implications for primary health care. BJOG 2015;122:312–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous