

Understanding decisions about antibiotic prescribing in ICU: an application of the Necessity Concerns Framework
- PMID: 34099497
- PMCID: PMC8899486
- DOI: 10.1136/bmjqs-2020-012479
Understanding decisions about antibiotic prescribing in ICU: an application of the Necessity Concerns Framework
Abstract
Background: Antibiotics are extensively prescribed in intensive care units (ICUs), yet little is known about how antibiotic-related decisions are made in this setting. We explored how beliefs, perceptions and contextual factors influenced ICU clinicians' antibiotic prescribing.
Methods: We conducted 4 focus groups and 34 semistructured interviews with clinicians involved in antibiotic prescribing in four English ICUs. Focus groups explored factors influencing prescribing, whereas interviews examined decision-making processes using two clinical vignettes. Data were analysed using thematic analysis, applying the Necessity Concerns Framework.
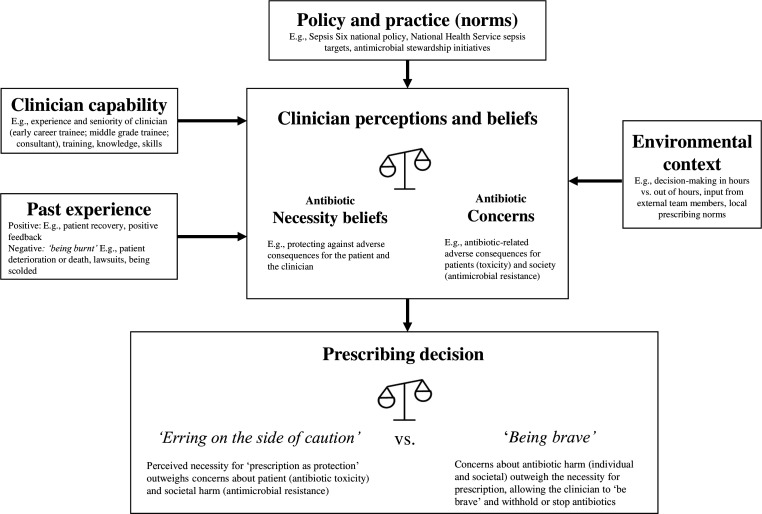
Results: Clinicians' antibiotic decisions were influenced by their judgement of the necessity for prescribing/not prescribing, relative to their concerns about potential adverse consequences. Antibiotic necessity perceptions were strongly influenced by beliefs that antibiotics would protect patients from deterioration and themselves from the ethical and legal consequences of undertreatment. Clinicians also reported concerns about prescribing antibiotics. These generally centred on antimicrobial resistance; however, protecting the individual patient was prioritised over these societal concerns. Few participants identified antibiotic toxicity concerns as a key influencer. Clinical uncertainty often complicated balancing antibiotic necessity against concerns. Decisions to start or continue antibiotics often represented 'erring on the side of caution' as a protective response in uncertainty. This approach was reinforced by previous experiences of negative consequences ('being burnt') which motivated prescribing 'just in case' of an infection. Prescribing decisions were also context-dependent, exemplified by a lower perceived threshold to prescribe antibiotics out-of-hours, input from external team members and local prescribing norms.
Conclusion: Efforts to improve antibiotic stewardship should consider clinicians' desire to protect with a prescription. Rapid molecular microbiology, with appropriate communication, may diminish clinicians' fears of not prescribing or of using narrower-spectrum antibiotics.
Keywords: antibiotic management; critical care; decision making; qualitative research.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: VIE reports personal fees and non-financial support from bioMerieux, personal fees from Curetis and non-financial support from Oxford Nanopore Technologies, outside the submitted work. DML reports personal fees from Accelerate, Allecra, Antabio, Astellas, Beckman Coulter, bioMerieux, Cepheid, Centauri, Entasis, Johnson & Johnson, Meiji, Melinta, Menarini, Mutabilis, Nordic, ParaPharm, QPEX, Roche, Shionogi, Tetraphase, Wockhardt, Zambon, Cardiome and Eumedica. He also reports grants and personal fees from VenatoRx; personal fees and other (shareholder) from GlaxoSmithKline; personal fees and other (stock options) from TAZ; grants, personal fees and other (shareholder) from Merck/MSD and Pfizer; and other (shareholder) from Perkin Elmer and Dechra. All are outside the submitted work.
Figures
Similar articles
-
Guidelines vs mindlines: a qualitative investigation of how clinicians' beliefs influence the application of rapid molecular diagnostics in intensive care.Antimicrob Agents Chemother. 2025 Mar 5;69(3):e0115624. doi: 10.1128/aac.01156-24. Epub 2025 Feb 5. Antimicrob Agents Chemother. 2025. PMID: 39907301 Free PMC article.
-
Intensivists' beliefs about rapid multiplex molecular diagnostic testing and its potential role in improving prescribing decisions and antimicrobial stewardship: a qualitative study.Antimicrob Resist Infect Control. 2021 Jun 29;10(1):95. doi: 10.1186/s13756-021-00961-4. Antimicrob Resist Infect Control. 2021. PMID: 34187563 Free PMC article.
-
Balancing the risks to individual and society: a systematic review and synthesis of qualitative research on antibiotic prescribing behaviour in hospitals.J Hosp Infect. 2019 Apr;101(4):428-439. doi: 10.1016/j.jhin.2018.08.007. Epub 2018 Aug 9. J Hosp Infect. 2019. PMID: 30099092
-
The inconvincible patient: how clinicians perceive demand for antibiotics in the outpatient setting.Fam Pract. 2020 Mar 25;37(2):276-282. doi: 10.1093/fampra/cmz066. Fam Pract. 2020. PMID: 31690948
-
Behavioral Economics and Ambulatory Antibiotic Stewardship: A Narrative Review.Clin Ther. 2021 Oct;43(10):1654-1667. doi: 10.1016/j.clinthera.2021.08.004. Epub 2021 Oct 23. Clin Ther. 2021. PMID: 34702589 Free PMC article. Review.
Cited by
-
Clinical, contextual and hospital-level factors associated with escalation and de-escalation of empiric Gram-negative antibiotics among US inpatients.JAC Antimicrob Resist. 2023 May 13;5(3):dlad054. doi: 10.1093/jacamr/dlad054. eCollection 2023 Jun. JAC Antimicrob Resist. 2023. PMID: 37193004 Free PMC article.
-
Point-of-care tests, diagnostic uncertainty and antimicrobial stewardship in the ICU: procalcitonin or PCR to aid antibiotic-stop decisions - an observational cohort study.BMJ Open. 2024 Dec 20;14(12):e084872. doi: 10.1136/bmjopen-2024-084872. BMJ Open. 2024. PMID: 39806620 Free PMC article.
-
Evaluation of appropriateness of antibiotic prescribing in primary healthcare institutions in China using proxy indicator.Lancet Reg Health West Pac. 2024 Jul 2;49:101132. doi: 10.1016/j.lanwpc.2024.101132. eCollection 2024 Aug. Lancet Reg Health West Pac. 2024. PMID: 39056089 Free PMC article.
-
Assessment of the appropriateness of antibiotic prescribing in an acute UK hospital using a national audit tool: a single centre retrospective survey.Eur J Hosp Pharm. 2024 Oct 25;31(6):505-510. doi: 10.1136/ejhpharm-2022-003569. Eur J Hosp Pharm. 2024. PMID: 37117009
-
The imperative of teamwork in antimicrobial stewardship (AMS) interventions: insights from an ethnographic study with practitioners in Spain.JAC Antimicrob Resist. 2024 Sep 3;6(5):dlae133. doi: 10.1093/jacamr/dlae133. eCollection 2024 Oct. JAC Antimicrob Resist. 2024. PMID: 39234217 Free PMC article. Review.
References
-
- Moore LSP, Freeman R, Gilchrist MJ, et al. . Homogeneity of antimicrobial policy, yet heterogeneity of antimicrobial resistance: antimicrobial non-susceptibility among 108,717 clinical isolates from primary, secondary and tertiary care patients in London. J Antimicrob Chemother 2014;69:3409–22. 10.1093/jac/dku307 - DOI - PMC - PubMed
-
- De Waele JJ, Akova M, Antonelli M, et al. . Antimicrobial resistance and antibiotic stewardship programs in the ICU: insistence and persistence in the fight against resistance. A position statement from ESICM/ESCMID/WAAAR round table on multi-drug resistance. Intensive Care Med 2018;44:189–96. 10.1007/s00134-017-5036-1 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical