

Latency, Anti-Bacterial Resistance Pattern, and Bacterial Infection-Related Glomerulonephritis
- PMID: 34099500
- PMCID: PMC8455032
- DOI: 10.2215/CJN.18631120
Latency, Anti-Bacterial Resistance Pattern, and Bacterial Infection-Related Glomerulonephritis
Abstract
Background and objectives: Bacterial infection-related GN occurs concurrent to or after known or unknown infections. It is important to understand the clinical implications of the bacterial isolates, antimicrobial resistance patterns, and effect of latency-based classification on kidney and patient outcomes.
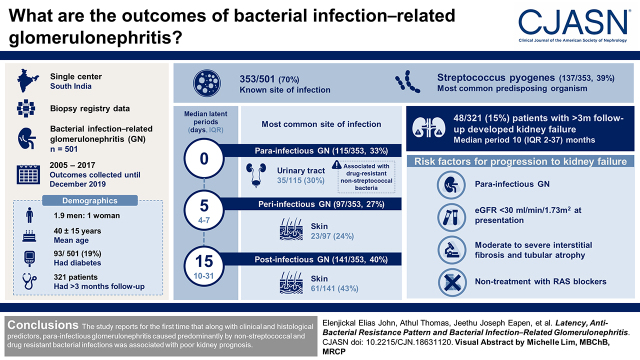
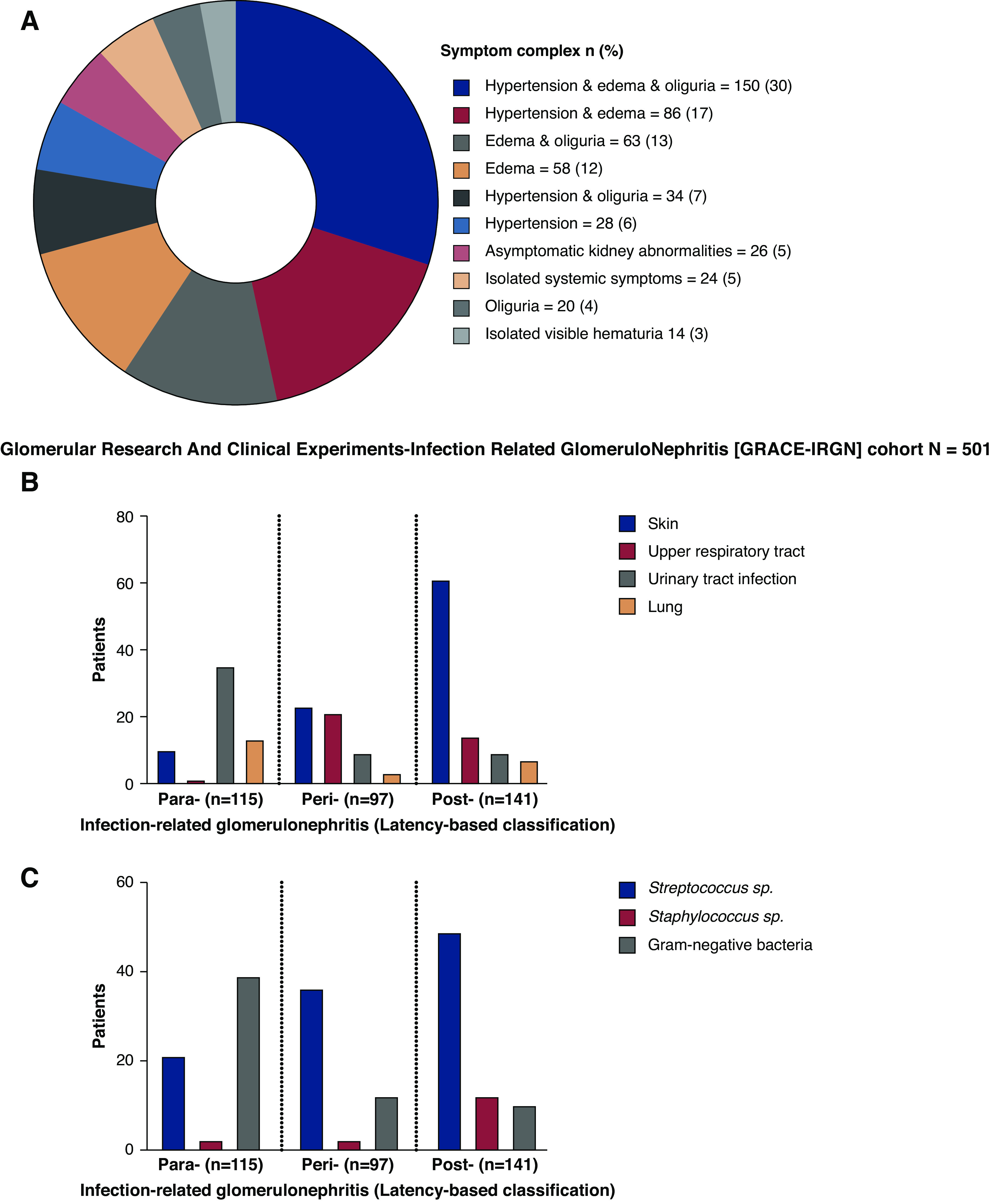
Design, setting, participants, & measurements: In total, 501 consecutive adults diagnosed with bacterial infection-related GN between 2005 and 2017 were included from a biopsy registry of 15,545 patients at a single center in South India, and follow-up data were collected from electronic medical records until December 2019. Latency was defined as time between resolution of infection and onset of GN, which was classified as parainfectious, peri-infectious, or postinfectious GN. Longitudinal kidney and patient outcomes were studied.
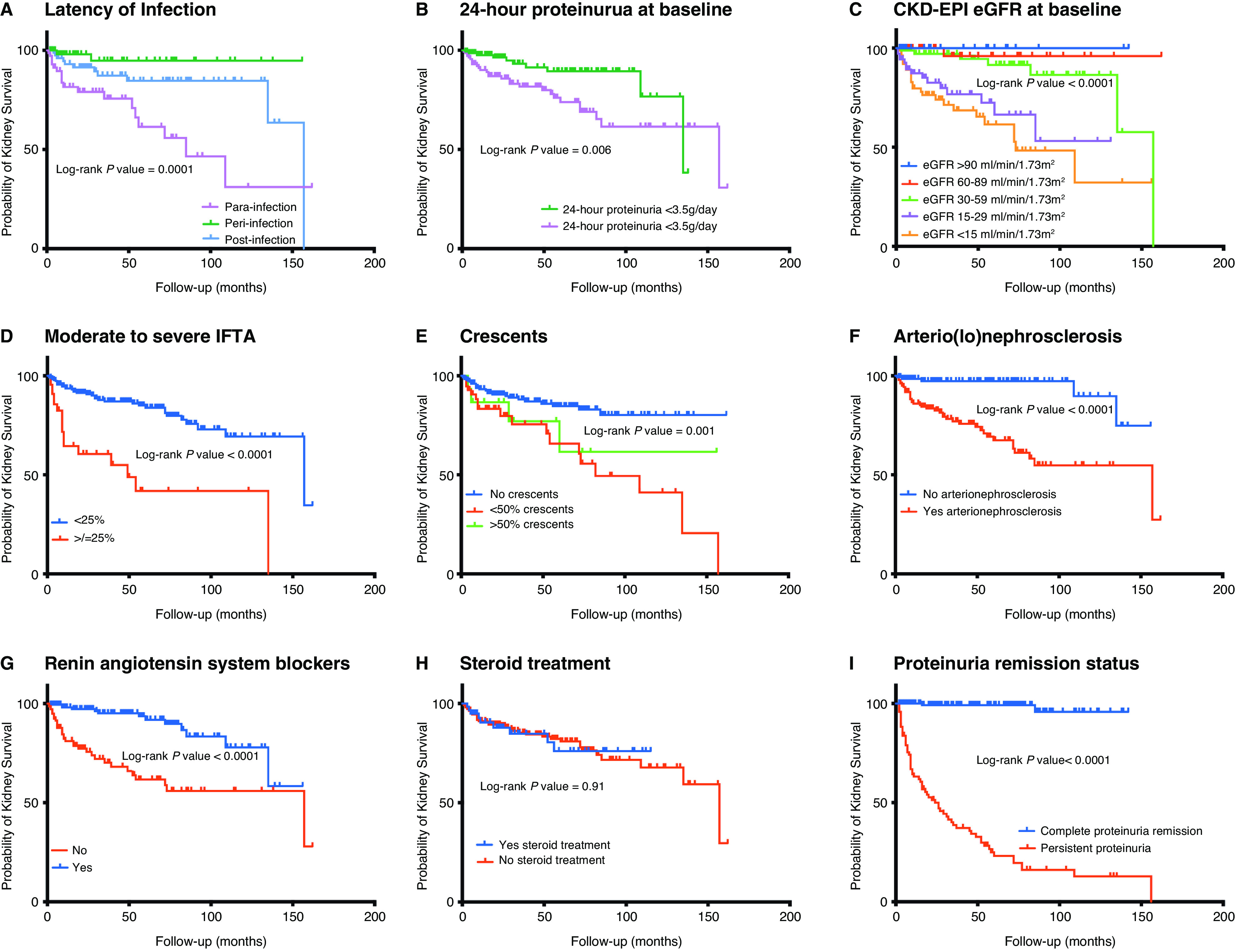
Results: The mean age of the cohort was 40 (± 15) years, 6% were above 65 years, and 330 (66%) were men. Diabetes was present in 93 (19%) patients. Seventy percent (353 of 501) of patients had known infections, with the median latent period for parainfectious (115 of 353, 33%), peri-infectious (97 of 353, 27%), and postinfectious (141 of 353, 40%) GN being 0, 5 (4-7), and 15 (10-31) days, respectively. The most common predisposing organism was Streptococcus pyogenes (137 of 353, 39%). Drug-resistant nonstreptococcal bacteria were methicillin-resistant Staphylococcus aureus (25%, four of 16), extended-spectrum β-lactamases (20%, 12 of 59), and carbapenem-resistant organisms (10%, six of 59). Twenty of 22 (91%) of the drug-resistant organisms were isolated from the parainfectious group. The most common site of infection was skin in peri- (23 of 97, 24%) and postinfectious GN (61 of 141, 43%), and urinary tract in parainfectious GN (35 of 115, 30%). Of 321 patients with >3 months of follow-up, 48 (15%) developed kidney failure over a median period of 10 (2-37) months and 14 (4%) died. Parainfectious GN, eGFR<30 ml/min per 1.73 m2, moderate-to-severe interstitial fibrosis and tubular atrophy, and nontreatment with renin-angiotensin system blockers were significant risk factors for progression to kidney failure by a Cox proportional-hazards model.
Conclusions: Along with clinical and histologic predictors, parainfectious GN caused predominantly by nonstreptococcal and drug-resistant bacterial infections was associated with poor kidney prognosis.
Keywords: bacterial infections; glomerular disease; immunology and pathology; kidney biopsy; nephritis; primary glomerulonephritis.
Copyright © 2021 by the American Society of Nephrology.
Figures
Comment in
-
New Insights into Epidemiology and Outcome of Bacterial Infection-Related Glomerulonephritis.Clin J Am Soc Nephrol. 2021 Aug;16(8):1149-1151. doi: 10.2215/CJN.07910621. Clin J Am Soc Nephrol. 2021. PMID: 34362782 Free PMC article. No abstract available.
Similar articles
-
Incidental healed postinfectious glomerulonephritis: a study of 1012 renal biopsy specimens examined by electron microscopy.Hum Pathol. 2003 Jan;34(1):3-10. doi: 10.1053/hupa.2003.53. Hum Pathol. 2003. PMID: 12605360
-
Predictors of Renal Outcomes in Sclerotic Class Anti-Neutrophil Cytoplasmic Antibody Glomerulonephritis.Am J Nephrol. 2018;48(6):465-471. doi: 10.1159/000494840. Epub 2018 Nov 23. Am J Nephrol. 2018. PMID: 30472700
-
Postinfectious glomerulonephritis--is there a link to alcoholism?Q J Med. 1994 Feb;87(2):97-102. Q J Med. 1994. PMID: 8153294
-
Epidemiology, pathogenesis, treatment and outcomes of infection-associated glomerulonephritis.Nat Rev Nephrol. 2020 Jan;16(1):32-50. doi: 10.1038/s41581-019-0178-8. Epub 2019 Aug 9. Nat Rev Nephrol. 2020. PMID: 31399725 Review.
-
New trends of an old disease: the acute post infectious glomerulonephritis at the beginning of the new millenium.J Nephrol. 2014 Jun;27(3):229-39. doi: 10.1007/s40620-013-0018-z. Epub 2014 Jan 31. J Nephrol. 2014. PMID: 24777751 Review.
Cited by
-
Bacterial infection-related glomerulonephritis in patients with diabetes.Nephrology (Carlton). 2023 Nov;28(11):597-610. doi: 10.1111/nep.14222. Epub 2023 Jul 26. Nephrology (Carlton). 2023. PMID: 37492933 Free PMC article.
-
Streptococcal Infection-related Glomerulonephritis in an Elderly Diabetic Patient Complicated by Hemophagocytic Syndrome and Cytomegalovirus Nephritis.Intern Med. 2023 Jan 15;62(2):261-267. doi: 10.2169/internalmedicine.9314-21. Epub 2022 Jun 28. Intern Med. 2023. PMID: 35768220 Free PMC article.
-
When to Suspect Non-diabetic Kidney Disease in a Diabetic Patient?Cureus. 2022 Aug 17;14(8):e28091. doi: 10.7759/cureus.28091. eCollection 2022 Aug. Cureus. 2022. PMID: 36158327 Free PMC article.
-
The Diagnostic Conundrum of Glomerular Crescents With IgA Deposits.Kidney Int Rep. 2022 Dec 31;8(3):507-518. doi: 10.1016/j.ekir.2022.12.024. eCollection 2023 Mar. Kidney Int Rep. 2022. PMID: 36938067 Free PMC article.
-
Emphysematous Pyelonephritis with IgA-Dominant Infection-Related Glomerulonephritis: An Unusual Picture.Acta Med Acad. 2022 Apr;51(1):59-63. doi: 10.5644/ama2006-124.371. Acta Med Acad. 2022. PMID: 35695404 Free PMC article.
References
-
- Nast CC: Infection-related glomerulonephritis: Changing demographics and outcomes. Adv Chronic Kidney Dis 19: 68–75, 2012 - PubMed
-
- Satoskar AA, Parikh SV, Nadasdy T: Epidemiology, pathogenesis, treatment and outcomes of infection-associated glomerulonephritis. Nat Rev Nephrol 16: 32–50, 2020 - PubMed
-
- Nasr SH, Radhakrishnan J, D’Agati VD: Bacterial infection-related glomerulonephritis in adults. Kidney Int 83: 792–803, 2013 - PubMed
-
- Glassock RJ, Alvarado A, Prosek J, Hebert C, Parikh S, Satoskar A, Nadasdy T, Forman J, Rovin B, Hebert LA: Staphylococcus-related glomerulonephritis and poststreptococcal glomerulonephritis: Why defining “post” is important in understanding and treating infection-related glomerulonephritis. Am J Kidney Dis 65: 826–832, 2015 - PubMed
-
- Nadasdy T, Hebert LA: Infection-related glomerulonephritis: Understanding mechanisms. Semin Nephrol 31: 369–375, 2011 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
