

Single-cell analyses of renal cell cancers reveal insights into tumor microenvironment, cell of origin, and therapy response
- PMID: 34099557
- PMCID: PMC8214680
- DOI: 10.1073/pnas.2103240118
Single-cell analyses of renal cell cancers reveal insights into tumor microenvironment, cell of origin, and therapy response
Abstract
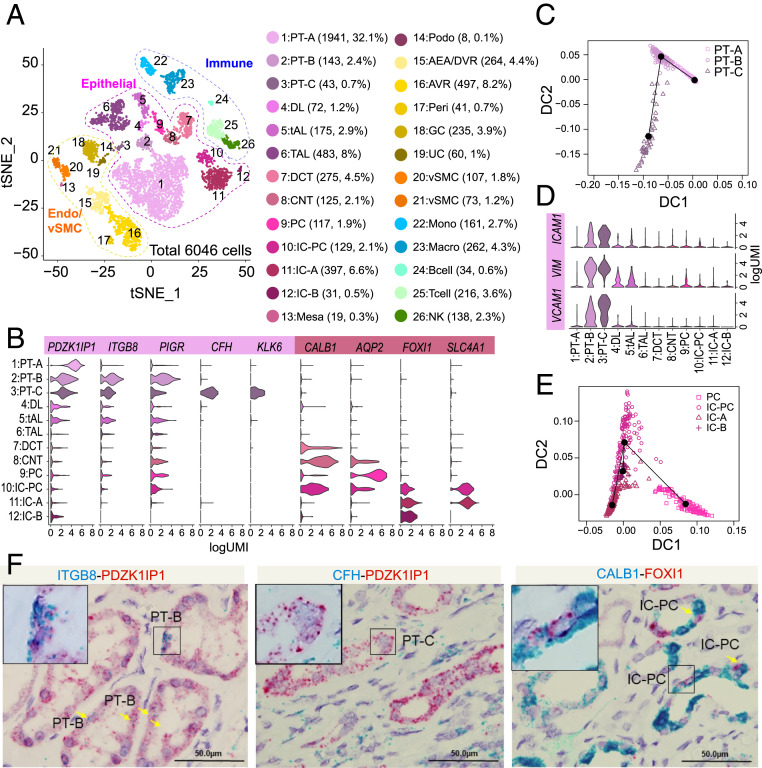
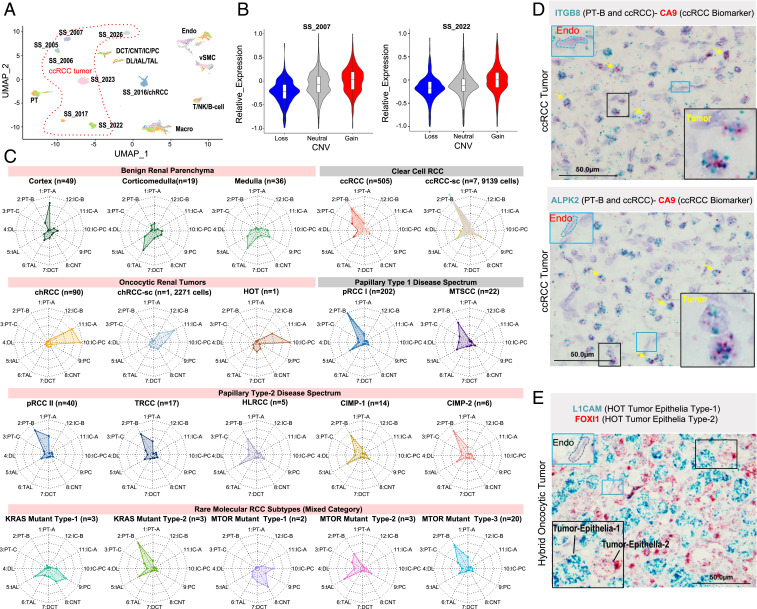
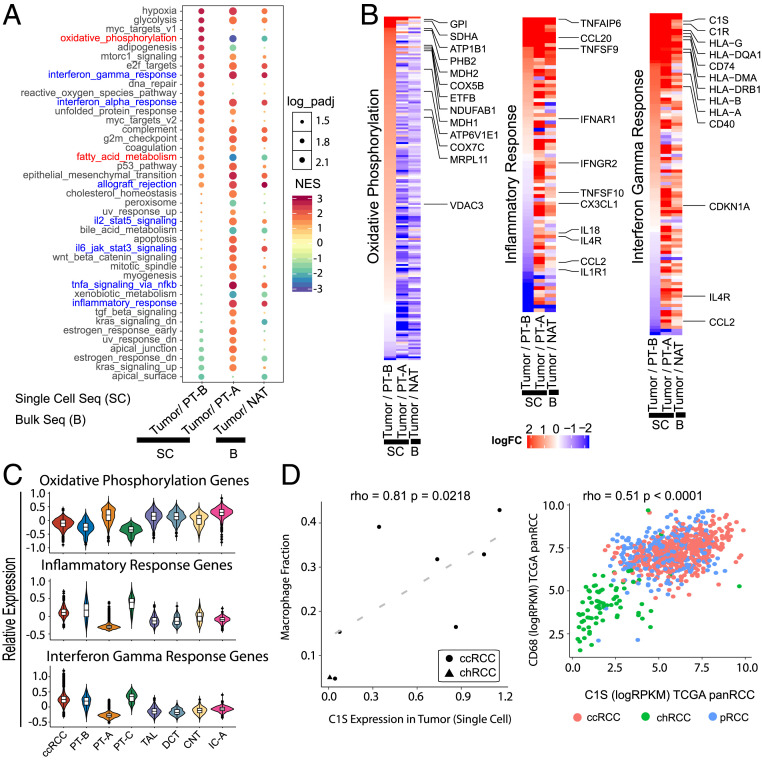
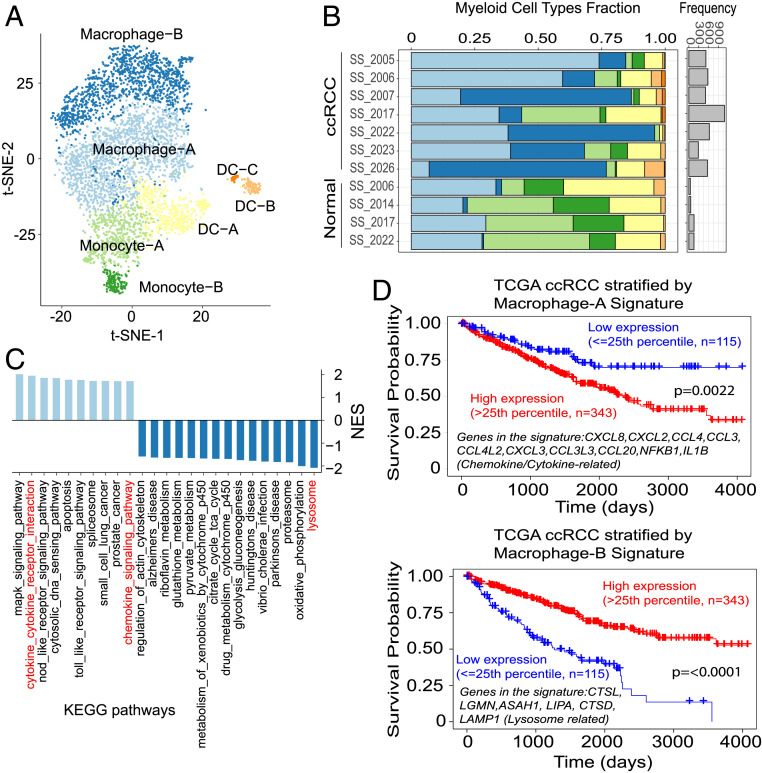
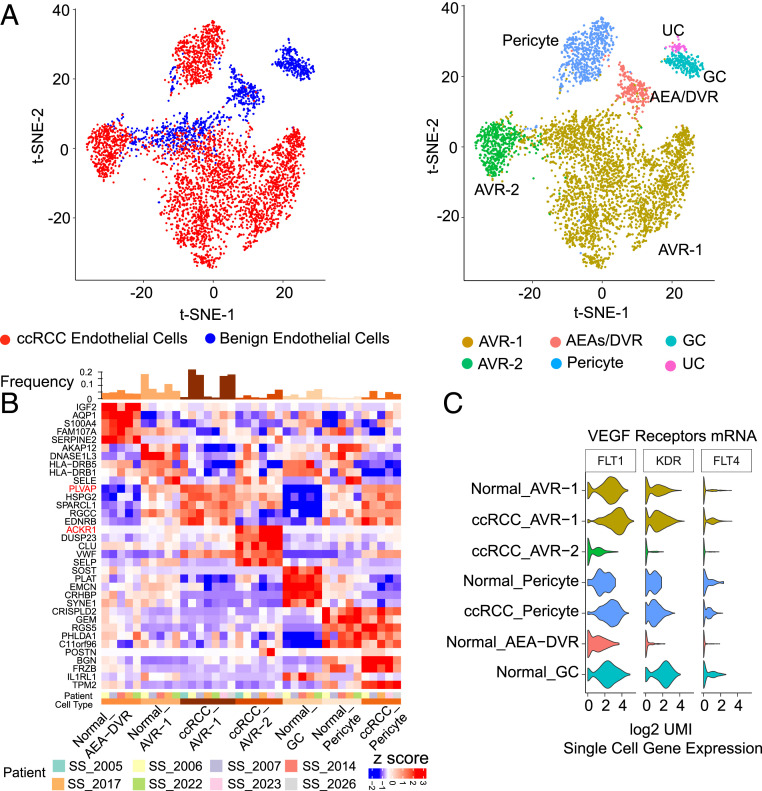
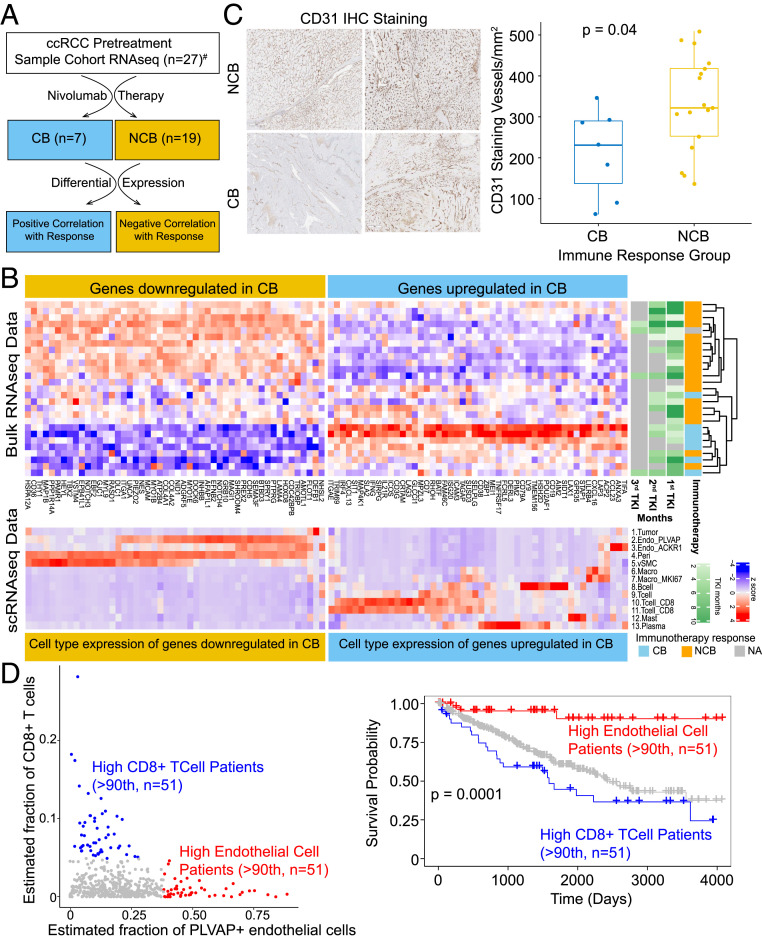
Diverse subtypes of renal cell carcinomas (RCCs) display a wide spectrum of histomorphologies, proteogenomic alterations, immune cell infiltration patterns, and clinical behavior. Delineating the cells of origin for different RCC subtypes will provide mechanistic insights into their diverse pathobiology. Here, we employed single-cell RNA sequencing (scRNA-seq) to develop benign and malignant renal cell atlases. Using a random forest model trained on this cell atlas, we predicted the putative cell of origin for more than 10 RCC subtypes. scRNA-seq also revealed several attributes of the tumor microenvironment in the most common subtype of kidney cancer, clear cell RCC (ccRCC). We elucidated an active role for tumor epithelia in promoting immune cell infiltration, potentially explaining why ccRCC responds to immune checkpoint inhibitors, despite having a low neoantigen burden. In addition, we characterized an association between high endothelial cell types and lack of response to immunotherapy in ccRCC. Taken together, these single-cell analyses of benign kidney and RCC provide insight into the putative cell of origin for RCC subtypes and highlight the important role of the tumor microenvironment in influencing ccRCC biology and response to therapy.
Keywords: cell of origin; clear cell renal cell carcinoma; renal cell carcinoma; single-cell RNA sequencing; tumor microenvironment.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
Competing interest statement: A.A. and P.M. are coauthors on an article [S. M. Esagian et al. BJU International, 10.1111/bju.15324 (2021)].
Figures
Similar articles
-
Landscape of immune cell infiltration in clear cell renal cell carcinoma to aid immunotherapy.Cancer Sci. 2021 Jun;112(6):2126-2139. doi: 10.1111/cas.14887. Epub 2021 Apr 7. Cancer Sci. 2021. PMID: 33735492 Free PMC article.
-
Integrated analysis of immune-related gene subtype and immune index for immunotherapy in clear cell renal cell carcinoma.Pathol Res Pract. 2021 Sep;225:153557. doi: 10.1016/j.prp.2021.153557. Epub 2021 Jul 20. Pathol Res Pract. 2021. PMID: 34329838
-
Construction of a Novel Immune-Related lncRNA Pair Signature with Prognostic Significance for Kidney Clear Cell Renal Cell Carcinoma.Dis Markers. 2021 Sep 1;2021:8800358. doi: 10.1155/2021/8800358. eCollection 2021. Dis Markers. 2021. PMID: 34512816 Free PMC article.
-
The immunology of renal cell carcinoma.Nat Rev Nephrol. 2020 Dec;16(12):721-735. doi: 10.1038/s41581-020-0316-3. Epub 2020 Jul 30. Nat Rev Nephrol. 2020. PMID: 32733094 Review.
-
The tumour microenvironment and metabolism in renal cell carcinoma targeted or immune therapy.J Cell Physiol. 2021 Mar;236(3):1616-1627. doi: 10.1002/jcp.29969. Epub 2020 Aug 11. J Cell Physiol. 2021. PMID: 32783202 Review.
Cited by
-
Metabolic heterogeneity in clear cell renal cell carcinoma revealed by single-cell RNA sequencing and spatial transcriptomics.J Transl Med. 2024 Feb 27;22(1):210. doi: 10.1186/s12967-024-04848-x. J Transl Med. 2024. PMID: 38414015 Free PMC article.
-
Toward a CRISPR-based mouse model of Vhl-deficient clear cell kidney cancer: Initial experience and lessons learned.Proc Natl Acad Sci U S A. 2024 Oct 8;121(41):e2408549121. doi: 10.1073/pnas.2408549121. Epub 2024 Oct 4. Proc Natl Acad Sci U S A. 2024. PMID: 39365820 Free PMC article.
-
Epigenetic regulation during cancer transitions across 11 tumour types.Nature. 2023 Nov;623(7986):432-441. doi: 10.1038/s41586-023-06682-5. Epub 2023 Nov 1. Nature. 2023. PMID: 37914932 Free PMC article.
-
Developmental Deconvolution for Classification of Cancer Origin.Cancer Discov. 2022 Nov 2;12(11):2566-2585. doi: 10.1158/2159-8290.CD-21-1443. Cancer Discov. 2022. PMID: 36041084 Free PMC article.
-
Development of prognostic signatures and risk index related to lipid metabolism in ccRCC.Front Oncol. 2024 Jun 13;14:1378095. doi: 10.3389/fonc.2024.1378095. eCollection 2024. Front Oncol. 2024. PMID: 38939337 Free PMC article.
References
-
- Udager A. M., Mehra R., Morphologic, molecular, and taxonomic evolution of renal cell carcinoma: A conceptual perspective with emphasis on updates to the 2016 World Health Organization classification. Arch. Pathol. Lab. Med. 140, 1026–1037 (2016). - PubMed
-
- Lindgren D., et al. ., Cell-type-specific gene programs of the normal human nephron define kidney cancer subtypes. Cell Rep. 20, 1476–1489 (2017). - PubMed
-
- Prasad S. R., et al. ., Segmental disorders of the nephron: Histopathological and imaging perspective. Br. J. Radiol. 80, 593–602 (2007). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
