

Implications of incidental findings from lung screening for primary care: data from a UK pilot
- PMID: 34099737
- PMCID: PMC8184811
- DOI: 10.1038/s41533-021-00246-8
Implications of incidental findings from lung screening for primary care: data from a UK pilot
Abstract
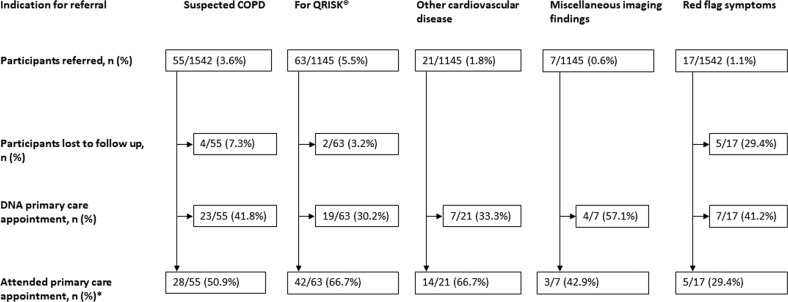
Regional lung cancer screening (LCS) is underway in England, involving a "lung health check" (LHC) and low-dose CT scan for those at high risk of cancer. Incidental findings from LHCs or CTs are usually referred to primary care. We describe the proportion of participants referred from the West London LCS pilot to primary care, the indications for referral, the number of general practitioner (GP) attendances and consequent changes to patient management, and provide an estimated cost-burden analysis for primary care. A small proportion (163/1542, 10.6%) of LHC attendees were referred to primary care, primarily for suspected undiagnosed chronic obstructive pulmonary disease (55/163, 33.7%) or for QRISK® (63/163, 38.7%) assessment. Ninety one of 159 (57.2%) participants consenting to follow-up attended GP appointments; costs incurred by primary care were estimated at £5.69/LHC participant. Patient management changes occurred in only 36/159 (22.6%) referred participants. LHCs result in a small increase to primary care workload provided a strict referral protocol is adhered to. Changes to patient management arising from incidental findings referrals are infrequent.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Crosbie PA, et al. Implementing lung cancer screening: baseline results from a community-based ‘Lung Health Check’ pilot in deprived areas of Manchester. Thorax. 2018;4:55–59. - PubMed
-
- Crosbie PA, et al. Yorkshire Lung Screening Trial (YLST): protocol for a randomised controlled trial to evaluate invitation to community-based low-dose CT screening for lung cancer versus usual care in a targeted population at risk. BMJ Open. 2020;10:e037075. doi: 10.1136/bmjopen-2020-037075. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
