

Corneal biomechanical parameters in keratoconus eyes with abnormal elevation on the back corneal surface only versus both back and front surfaces
- PMID: 34099765
- PMCID: PMC8184812
- DOI: 10.1038/s41598-021-91263-7
Corneal biomechanical parameters in keratoconus eyes with abnormal elevation on the back corneal surface only versus both back and front surfaces
Abstract
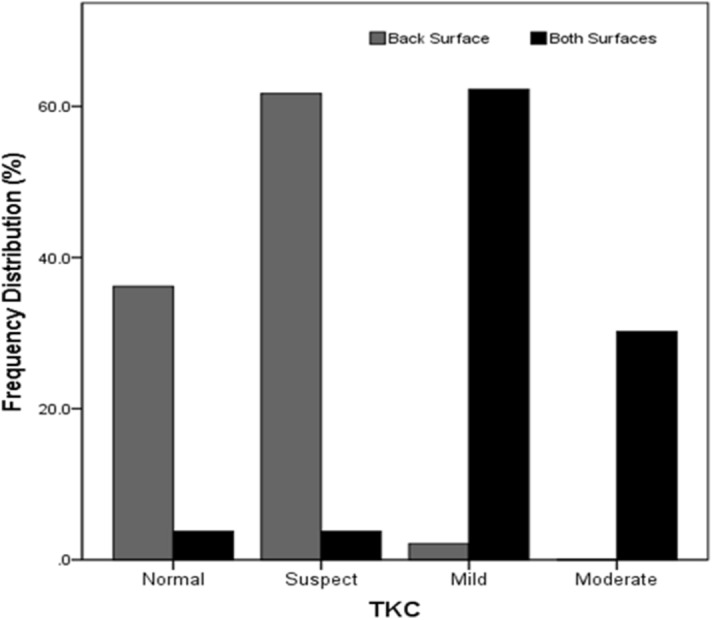
Corneal biomechanical parameters were compared in 100 keratoconus eyes with abnormal elevation on the back corneal surface only (group 1), versus both the back and front surfaces (group 2). Scheimpflug tomography with Pentacam HR, corneal biomechanical assessments using Corvis ST and Ocular Response Analyzer (ORA) and corneal epithelium thickness maps using anterior segment optical coherence tomography were assessed. There were no significant differences in the IOP measured using Corvis ST and ORA, age or sex between the two groups. Statistically significant differences were found in all corneal shape parameters and all new parameters of Corvis ST: corneal stiffness parameter at first applanation (SP-A1), integrated inverse radius (IR) and deformation amplitude ratio (DAR)) between groups (p < 0.001). The classic parameters of ORA including corneal hysteresis (CH) and corneal resistance factor (CRF) were about 1.00 mmHg higher in group 1 (p < 0.001). In conclusion, keratoconus eyes with abnormal elevation limited to the back corneal surface have lower grade, stiffer corneal biomechanical parameters and less asymmetric shape. This is consistent with progressive biomechanical weakening from the first detectable back surface elevation to manifestation on the front surface as the severity overwhelms the ability of the epithelium to compensate.
Conflict of interest statement
Drs Roberts and Ambrósio are consultants for Oculus. No conflicting relationship exists for other authors.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
