

Ibrutinib does not prevent kidney fibrosis following acute and chronic injury
- PMID: 34099830
- PMCID: PMC8184891
- DOI: 10.1038/s41598-021-91491-x
Ibrutinib does not prevent kidney fibrosis following acute and chronic injury
Abstract
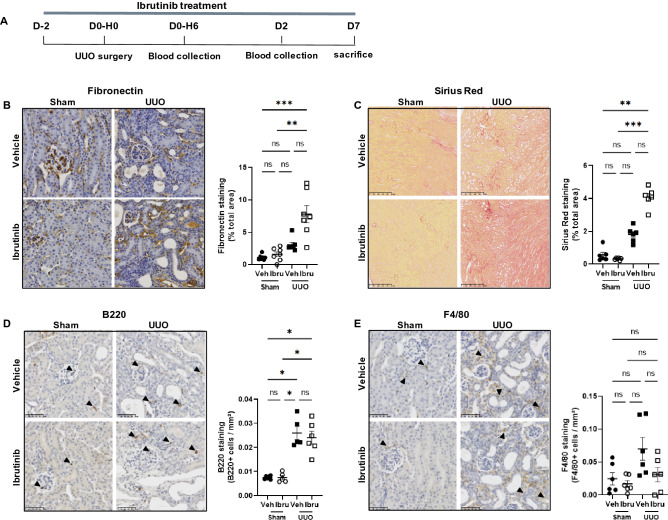
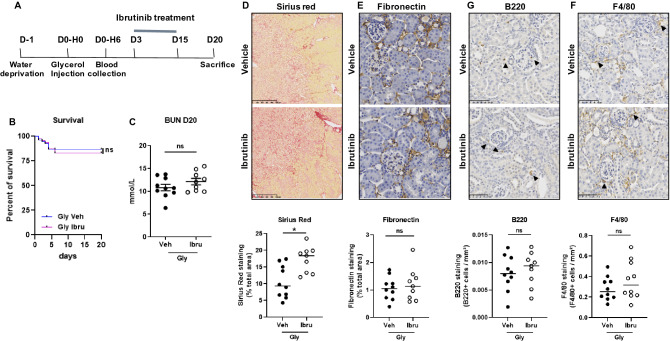
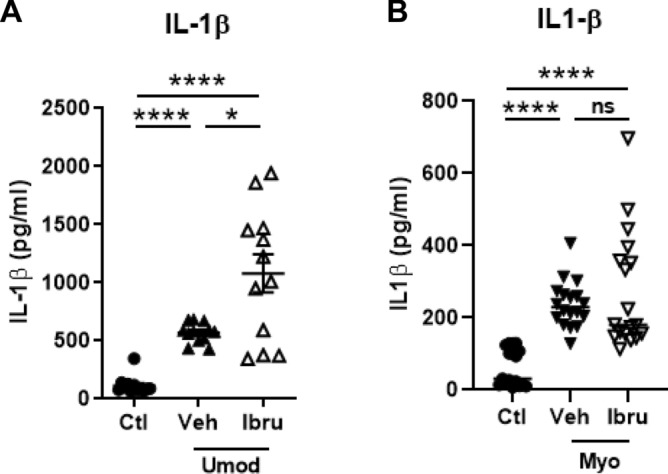
Recent studies suggested that ibrutinib, a Bruton tyrosine kinase (BTK) inhibitor, developed for the treatment of chronic lymphocytic leukemia, may prevent NLRP3 inflammasome activation in macrophages, IL-1β secretion and subsequent development of inflammation and organ fibrosis. The role of NLRP3 has been underlined in the various causes of acute kidney injury (AKI), a pathology characterized by high morbimortality and risk of transition toward chronic kidney disease (CKD). We therefore hypothesized that the BTK-inhibitor ibrutinib could be a candidate drug for AKI treatment. Here, we observed in both an AKI model (glycerol-induced rhabdomyolysis) and a model of rapidly progressive kidney fibrosis (unilateral ureteral obstruction), that ibrutinib did not prevent inflammatory cell recruitment in the kidney and fibrosis. Moreover, ibrutinib pre-exposure led to high mortality rate owing to severer rhabdomyolysis and AKI. In vitro, ibrutinib potentiated or had no effect on the secretion of IL-1β by monocytes exposed to uromodulin or myoglobin, two danger-associated molecule patterns proteins involved in the AKI to CKD transition. According to these results, ibrutinib should not be considered a candidate drug for patients developing AKI.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
