

Effect of competing mortality risks on predictive performance of the QRISK3 cardiovascular risk prediction tool in older people and those with comorbidity: external validation population cohort study
- PMID: 34100008
- PMCID: PMC8175241
- DOI: 10.1016/S2666-7568(21)00088-X
Effect of competing mortality risks on predictive performance of the QRISK3 cardiovascular risk prediction tool in older people and those with comorbidity: external validation population cohort study
Erratum in
-
Correction to Lancet Healthy Longev 2021; 2: e352-61.Lancet Healthy Longev. 2021 Aug;2(8):e458. doi: 10.1016/S2666-7568(21)00185-9. Lancet Healthy Longev. 2021. PMID: 34435191 Free PMC article.
Abstract
Background: Primary prevention of cardiovascular disease (CVD) is guided by risk-prediction tools, but these rarely account for the risk of dying from other conditions (ie, competing mortality risk). In England and Wales, the recommended risk-prediction tool is QRISK2, and a new version (QRISK3) has been derived and internally validated. We aimed to externally validate QRISK3 and to assess the effects of competing mortality risk on its predictive performance.
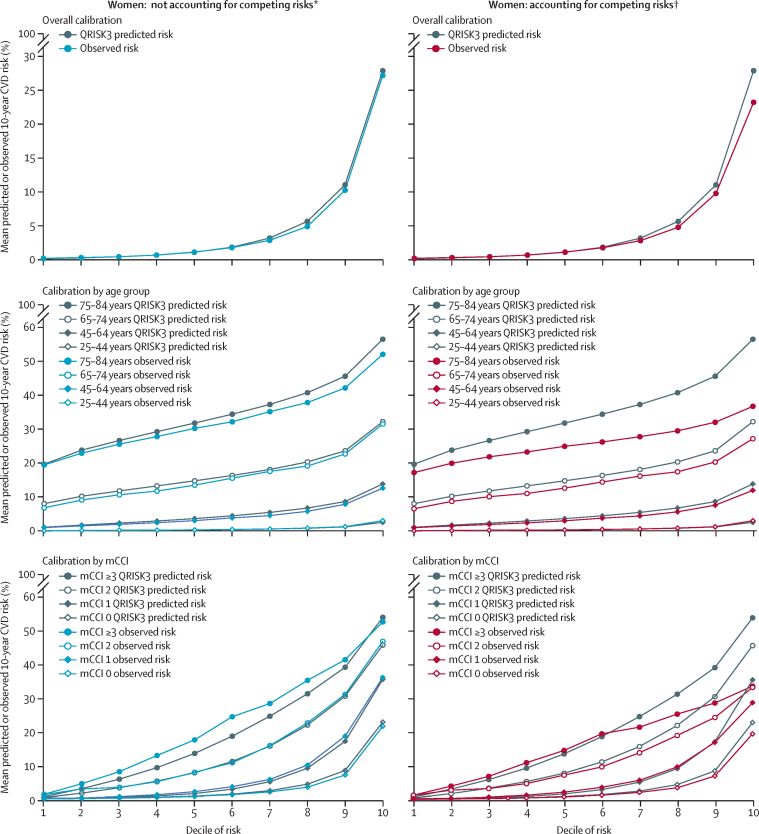
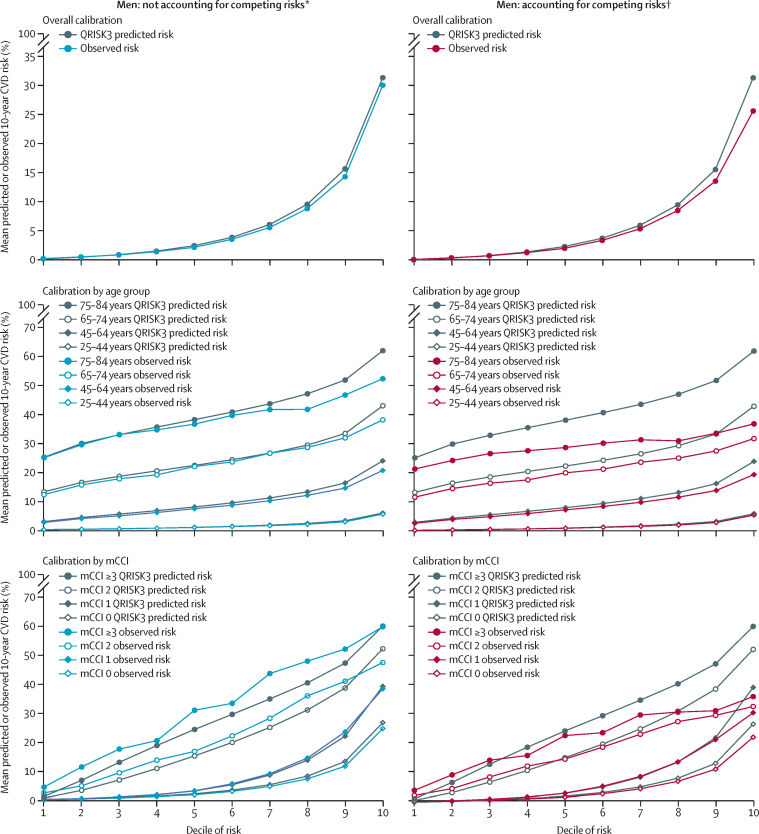
Methods: For this retrospective population cohort study, we used data from the Clinical Practice Research Datalink. We included patients aged 25-84 years with no previous history of CVD or statin treatment who were permanently registered with a primary care practice, had up-to-standard data for at least 1 year, and had linkage to Hospital Episode Statistics discharge and Office of National Statistics mortality data. We compared the QRISK3-predicted 10-year CVD risk with the observed 10-year risk in the whole population and in important subgroups of age and multimorbidity. QRISK3 discrimination and calibration were examined with and without accounting for competing risks.
Findings: Our study population included 1 484 597 women with 42 451 incident CVD events (4·9 cases per 1000 person-years of follow-up, 95% CI 4·89-4·99), and 1 420 176 men with 53 066 incident CVD events (6·7 cases per 1000 person-years, 6·66-6·78), with median follow-up of 5·0 years (IQR 1·9-9·2). Non-CVD death rose markedly with age (0·4% of women and 0·5% of men aged 25-44 years had a non-CVD death vs 20·1% of women and 19·6% of men aged 75-84 years). QRISK3 discrimination in the whole population was excellent (Harrell's C-statistic 0·865 in women and 0·834 in men) but was poor in older age groups (<0·65 in all subgroups aged 65 years or older). Ignoring competing risks, QRISK3 calibration in the whole population and in younger people was excellent, but there was significant over-prediction in older people. Accounting for competing risks, QRISK3 systematically over-predicted CVD risk, particularly in older people and in those with high multimorbidity.
Interpretation: QRISK3 performed well at the whole population level when ignoring competing mortality risk. The tool performed considerably less well in important subgroups, including older people and people with multimorbidity, and less well again after accounting for competing mortality risk.
Funding: National Institute for Health Research.
© 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license.
Conflict of interest statement
PTD reports a grant from AbbVie, outside the submitted work, and is a member of the NHS Scottish Medicines Consortium. J-HY is currently employed by ICON PLC Clinical Research. DRM reports grants from the Chief Scientist Office, Health Data Research UK, and National Institute for Health Research, outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Challenges of treating cardiovascular risk in old age.Lancet Healthy Longev. 2021 Jun;2(6):e308-e309. doi: 10.1016/S2666-7568(21)00114-8. Epub 2021 Jun 3. Lancet Healthy Longev. 2021. PMID: 36098141 No abstract available.
Similar articles
-
Predictive performance of a competing risk cardiovascular prediction tool CRISK compared to QRISK3 in older people and those with comorbidity: population cohort study.BMC Med. 2022 May 4;20(1):152. doi: 10.1186/s12916-022-02349-6. BMC Med. 2022. PMID: 35505353 Free PMC article.
-
The implications of competing risks and direct treatment disutility in cardiovascular disease and osteoporotic fracture: risk prediction and cost effectiveness analysis.Health Soc Care Deliv Res. 2024 Feb;12(4):1-275. doi: 10.3310/KLTR7714. Health Soc Care Deliv Res. 2024. PMID: 38420962
-
External validation of the QLifetime cardiovascular risk prediction tool: population cohort study.BMC Cardiovasc Disord. 2023 Apr 15;23(1):194. doi: 10.1186/s12872-023-03209-8. BMC Cardiovasc Disord. 2023. PMID: 37061672 Free PMC article.
-
Nontraditional Risk Factors in Cardiovascular Disease Risk Assessment: A Systematic Evidence Report for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Jul. Report No.: 17-05225-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Jul. Report No.: 17-05225-EF-1. PMID: 30234933 Free Books & Documents. Review.
-
Performance of prediction models for nephropathy in people with type 2 diabetes: systematic review and external validation study.BMJ. 2021 Sep 28;374:n2134. doi: 10.1136/bmj.n2134. BMJ. 2021. PMID: 34583929 Free PMC article.
Cited by
-
Predictive value of metabolic profiling in cardiovascular risk scores: analysis of 75 000 adults in UK Biobank.J Epidemiol Community Health. 2023 Dec;77(12):802-808. doi: 10.1136/jech-2023-220801. Epub 2023 Sep 12. J Epidemiol Community Health. 2023. PMID: 37699667 Free PMC article.
-
Stroke risk in older British men: Comparing performance of stroke-specific and composite-CVD risk prediction tools.Prev Med Rep. 2022 Dec 24;31:102098. doi: 10.1016/j.pmedr.2022.102098. eCollection 2023 Feb. Prev Med Rep. 2022. PMID: 36820364 Free PMC article.
-
Prevalence and Clinical Correlates of Radiologically Detected Coronary Artery Disease in Chronic Obstructive Pulmonary Disease: A Cross-Sectional Observational Study.Am J Respir Crit Care Med. 2025 Jun;211(6):946-956. doi: 10.1164/rccm.202404-0838OC. Am J Respir Crit Care Med. 2025. PMID: 39680915
-
Feasibility of multiorgan risk prediction with routinely collected diagnostics: a prospective cohort study in the UK Biobank.BMJ Evid Based Med. 2024 Sep 20;29(5):313-323. doi: 10.1136/bmjebm-2023-112518. BMJ Evid Based Med. 2024. PMID: 38719437 Free PMC article.
-
Cardiovascular Risk and Plasma N-terminal Pro-B-type Natriuretic Peptide in Adults With Resistance to Thyroid Hormone β.J Endocr Soc. 2025 Feb 11;9(4):bvaf023. doi: 10.1210/jendso/bvaf023. eCollection 2025 Mar 3. J Endocr Soc. 2025. PMID: 40065989 Free PMC article.
References
-
- National Institute for Health and Care Excellence . National Institute for Health and Care Excellence; London: 2014. Clinical Guideline 181: lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. 2014;129(suppl 2):S1–S45. - PubMed
-
- Steyerberg E. Springer; New York: 2009. Clinical prediction models: a practical approach to development, validation, and updating.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
