

This is a preprint.
SARS-CoV-2 Infects Syncytiotrophoblast and Activates Inflammatory Responses in the Placenta
- PMID: 34100019
- PMCID: PMC8183016
- DOI: 10.1101/2021.06.01.446676
SARS-CoV-2 Infects Syncytiotrophoblast and Activates Inflammatory Responses in the Placenta
Update in
-
Inflammatory responses in the placenta upon SARS-CoV-2 infection late in pregnancy.iScience. 2022 May 20;25(5):104223. doi: 10.1016/j.isci.2022.104223. Epub 2022 Apr 11. iScience. 2022. PMID: 35434541 Free PMC article.
Abstract
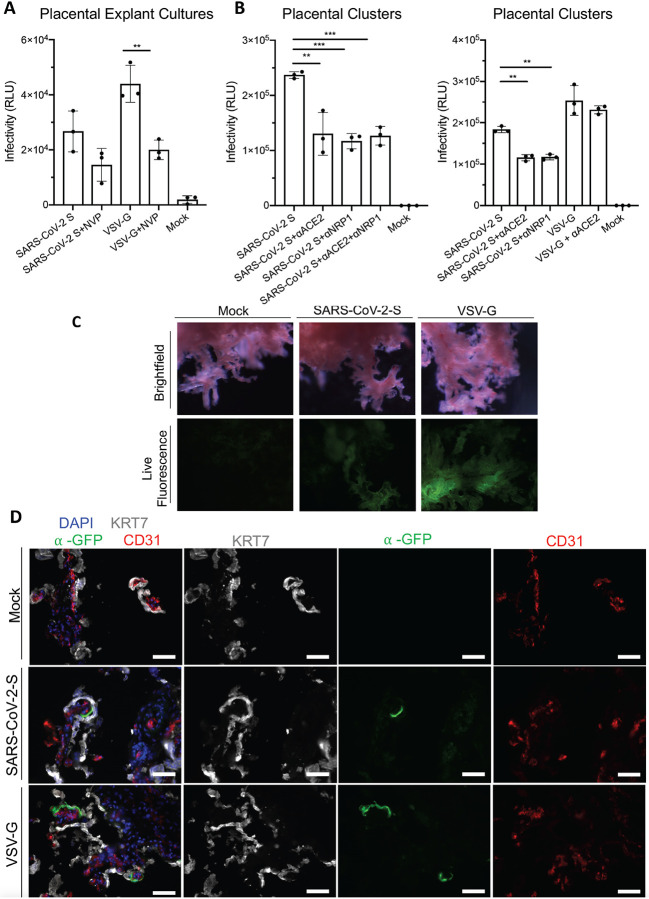
SARS-CoV-2 infection during pregnancy leads to an increased risk of adverse pregnancy outcomes. Although the placenta itself can be a target of virus infection, most neonates are virus free and are born healthy or recover quickly. Here, we investigated the impact of SARS-CoV-2 infection on the placenta from a cohort of women who were infected late during pregnancy and had tested nasal swab positive for SARS-CoV-2 by qRT-PCR at delivery. SARS-CoV-2 genomic and subgenomic RNA was detected in 23 out of 54 placentas. Two placentas with high virus content were obtained from mothers who presented with severe COVID-19 and whose pregnancies resulted in adverse outcomes for the fetuses, including intrauterine fetal demise and a preterm delivered baby still in newborn intensive care. Examination of the placental samples with high virus content showed efficient SARS-CoV-2 infection, using RNA in situ hybridization to detect genomic and replicating viral RNA, and immunohistochemistry to detect SARS-CoV-2 nucleocapsid protein. Infection was restricted to syncytiotrophoblast cells that envelope the fetal chorionic villi and are in direct contact with maternal blood. The infected placentas displayed massive infiltration of maternal immune cells including macrophages into intervillous spaces, potentially contributing to inflammation of the tissue. Ex vivo infection of placental cultures with SARS-CoV-2 or with SARS-CoV-2 spike (S) protein pseudotyped lentivirus targeted mostly syncytiotrophoblast and in rare events endothelial cells. Infection was reduced by using blocking antibodies against ACE2 and against Neuropilin 1, suggesting that SARS-CoV-2 may utilize alternative receptors for entry into placental cells.
Conflict of interest statement
Competing Interests R.E.S. is on the scientific advisory board of Miromatrix Inc and is a consultant and speaker for Alnylam Inc.
Figures


References
-
- Alamar I., Abu-Arja M. H., Heyman T., Roberts D. J., Desai N., Narula P., and Dygulska B.. 2020. ‘A Possible Case of Vertical Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in a Newborn With Positive Placental In Situ Hybridization of SARS-CoV-2 RNA’, J Pediatric Infect Dis Soc, 9: 636–39. - PMC - PubMed
-
- Arad A., Nammouz S., Nov Y., Ohel G., Bejar J., and Vadasz Z.. 2017. ‘The Expression of Neuropilin-1 in Human Placentas From Normal and Preeclamptic Pregnancies’, Int J Gynecol Pathol, 36: 42–49. - PubMed
-
- Baston-Buest D. M., Porn A. C., Schanz A., Kruessel J. S., Janni W., and Hess A. P.. 2011. ‘Expression of the vascular endothelial growth factor receptor neuropilin-1 at the human embryo-maternal interface’, Eur J Obstet Gynecol Reprod Biol, 154: 151–6. - PubMed
-
- Blanco-Melo D., Nilsson-Payant B. E., Liu W. C., Uhl S., Hoagland D., Møller R., Jordan T. X., Oishi K., Panis M., Sachs D., Wang T. T., Schwartz R. E., Lim J. K., Albrecht R. A., and tenOever B. R.. 2020. ‘Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19’, Cell, 181: 1036–45.e9. - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous