

Transcatheter Mitral Valve Repair Simulator Equipped with Eye Tracking Based Performance Assessment Capabilities: A Pilot Study
- PMID: 34100226
- PMCID: PMC8481152
- DOI: 10.1007/s13239-021-00549-4
Transcatheter Mitral Valve Repair Simulator Equipped with Eye Tracking Based Performance Assessment Capabilities: A Pilot Study
Abstract
Background: The increase in cardiovascular disease cases that require minimally invasive treatment is inducing a new need to train physicians to perform them safely and effectively. Nevertheless, adaptation to simulation-based training has been slow, especially for complex procedures.
Objectives: We describe a newly developed mitral valve repair (MVR) simulator, equipped with new objective performance assessment methods, with an emphasis on its use for training the MitraClip™ procedure.
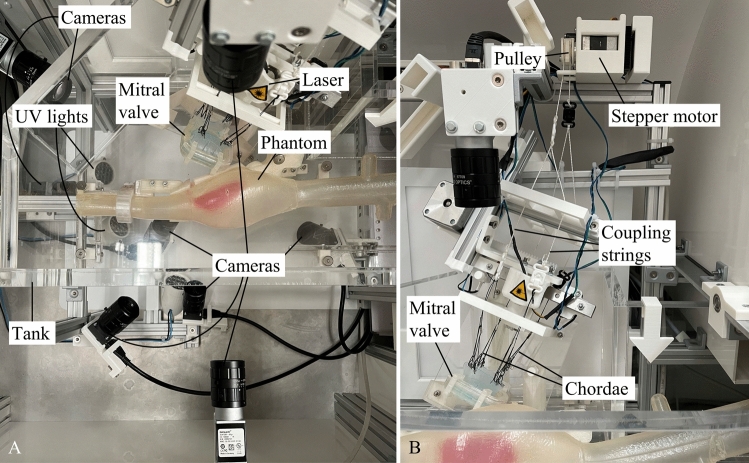
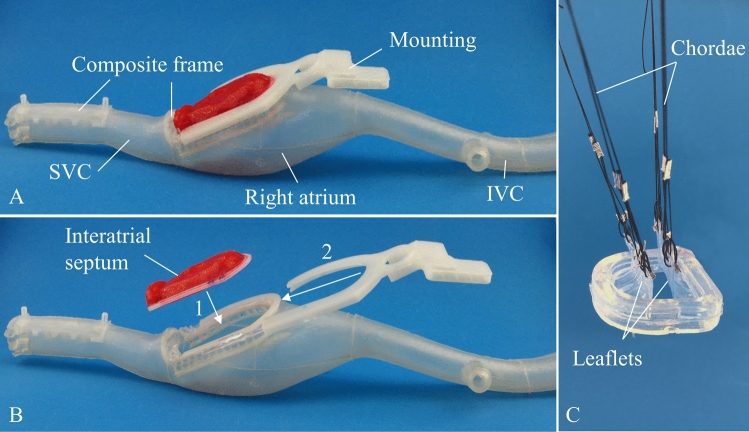
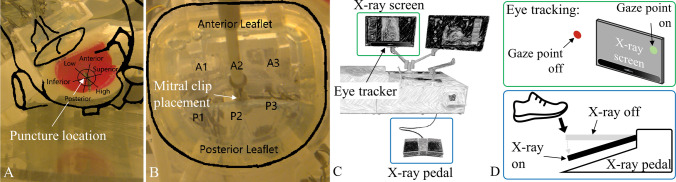
Methods: The MVR contains phantoms of all anatomical structures encountered during mitral valve repair with a transvenous, transseptal approach. In addition, several cameras, line lasers, and ultraviolet lights are used to mimic echocardiographic and fluoroscopic imaging and with a remote eye tracker the cognitive behaviour of the operator is recorded. A pilot study with a total of 9 interventional cardiologists, cardiac surgeons and technical experts was conducted. All participants performed the MitraClip procedure on the MVR simulator using standard interventional tools. Subsequently, each participant completed a structured questionnaire to assess the simulator.
Results: The simulator functioned well, and the implemented objective performance assessment methods worked reliably. Key performance metrics such as x-ray usage were comparable with results from studies assessing these metrics in real interventions. Fluoroscopy imaging is realistic for the transseptal puncture but reaches its limits during the final steps of the procedure.
Conclusion: The functionality and objective performance assessment of the MVR simulator were demonstrated. Especially for complex procedures such as the MitraClip procedure, this simulator offers a suitable platform for risk-free training and education.
Keywords: Education; MitraClip; Mitral valve; Objective assessment; Simulation training; Transseptal puncture.
© 2021. The Author(s).
Figures



References
-
- Chhatriwalla AK, Vemulapalli S, Holmes DR, Dai D, Li Z, Ailawadi G, Glower D, Kar S, Mack MJ, Rymer J, Kosinski AS, Sorajja P. Institutional experience with transcatheter mitral valve repair and clinical outcomes. JACC Cardiovasc. Interv. 2019;12:1342–1352. doi: 10.1016/j.jcin.2019.02.039. - DOI - PubMed
-
- Gong, R.H., B. Jenkins, R.W. Sze, Z. Yaniv. A cost effective and high fidelity fluoroscopy simulator using the Image-Guided Surgery Toolkit (IGSTK), 2014, vol. 903618, p. 903618.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
