

Deep Learning Application for Vocal Fold Disease Prediction Through Voice Recognition: Preliminary Development Study
- PMID: 34100770
- PMCID: PMC8241431
- DOI: 10.2196/25247
Deep Learning Application for Vocal Fold Disease Prediction Through Voice Recognition: Preliminary Development Study
Abstract
Background: Dysphonia influences the quality of life by interfering with communication. However, a laryngoscopic examination is expensive and not readily accessible in primary care units. Experienced laryngologists are required to achieve an accurate diagnosis.
Objective: This study sought to detect various vocal fold diseases through pathological voice recognition using artificial intelligence.
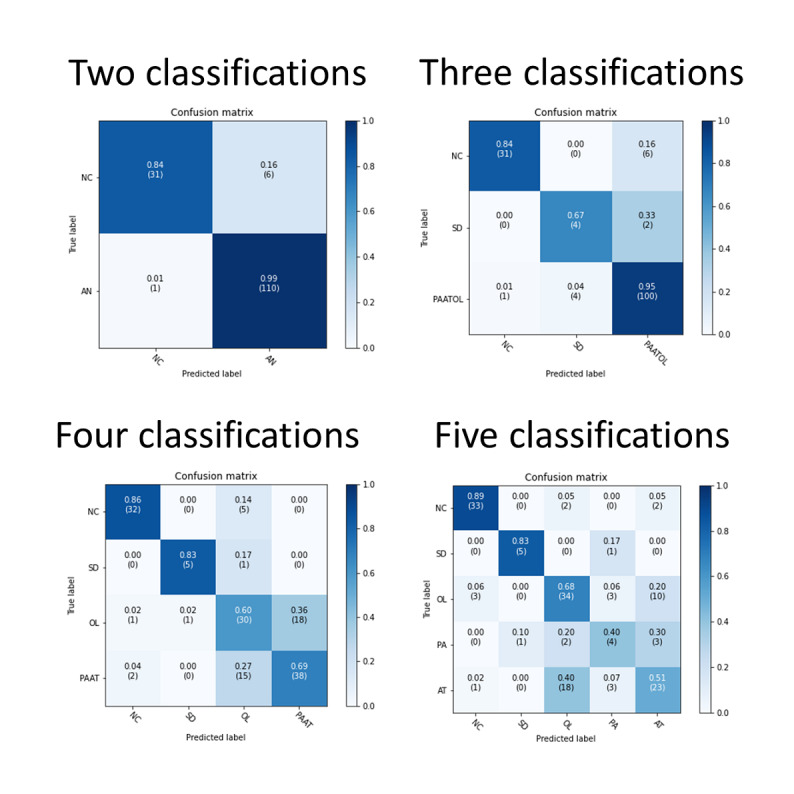
Methods: We collected 189 normal voice samples and 552 samples of individuals with voice disorders, including vocal atrophy (n=224), unilateral vocal paralysis (n=50), organic vocal fold lesions (n=248), and adductor spasmodic dysphonia (n=30). The 741 samples were divided into 2 sets: 593 samples as the training set and 148 samples as the testing set. A convolutional neural network approach was applied to train the model, and findings were compared with those of human specialists.
Results: The convolutional neural network model achieved a sensitivity of 0.66, a specificity of 0.91, and an overall accuracy of 66.9% for distinguishing normal voice, vocal atrophy, unilateral vocal paralysis, organic vocal fold lesions, and adductor spasmodic dysphonia. Compared with the accuracy of human specialists, the overall accuracy rates were 60.1% and 56.1% for the 2 laryngologists and 51.4% and 43.2% for the 2 general ear, nose, and throat doctors.
Conclusions: Voice alone could be used for common vocal fold disease recognition through a deep learning approach after training with our Mandarin pathological voice database. This approach involving artificial intelligence could be clinically useful for screening general vocal fold disease using the voice. The approach includes a quick survey and a general health examination. It can be applied during telemedicine in areas with primary care units lacking laryngoscopic abilities. It could support physicians when prescreening cases by allowing for invasive examinations to be performed only for cases involving problems with automatic recognition or listening and for professional analyses of other clinical examination results that reveal doubts about the presence of pathologies.
Keywords: artificial intelligence; convolutional neural network; dysphonia; pathological voice; vocal fold disease; voice pathology identification.
©Hao-Chun Hu, Shyue-Yih Chang, Chuen-Heng Wang, Kai-Jun Li, Hsiao-Yun Cho, Yi-Ting Chen, Chang-Jung Lu, Tzu-Pei Tsai, Oscar Kuang-Sheng Lee. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 08.06.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures



Similar articles
-
Detection of Pathological Voice Using Cepstrum Vectors: A Deep Learning Approach.J Voice. 2019 Sep;33(5):634-641. doi: 10.1016/j.jvoice.2018.02.003. Epub 2018 Mar 19. J Voice. 2019. PMID: 29567049
-
Developing an Artificial Intelligence Tool to Predict Vocal Cord Pathology in Primary Care Settings.Laryngoscope. 2023 Aug;133(8):1952-1960. doi: 10.1002/lary.30432. Epub 2022 Oct 13. Laryngoscope. 2023. PMID: 36226791
-
The effect of unilateral thalamic deep brain stimulation on the vocal dysfunction in a patient with spasmodic dysphonia: interrogating cerebellar and pallidal neural circuits.J Neurosurg. 2018 Feb;128(2):575-582. doi: 10.3171/2016.10.JNS161025. Epub 2017 Mar 17. J Neurosurg. 2018. PMID: 28304188 Clinical Trial.
-
Deep learning in voice analysis for diagnosing vocal cord pathologies: a systematic review.Eur Arch Otorhinolaryngol. 2024 Feb;281(2):863-871. doi: 10.1007/s00405-023-08362-6. Epub 2023 Dec 13. Eur Arch Otorhinolaryngol. 2024. PMID: 38091100
-
Is voice therapy effective for the treatment of dysphonic patients with benign vocal fold lesions?Auris Nasus Larynx. 2018 Aug;45(4):661-666. doi: 10.1016/j.anl.2017.08.003. Epub 2017 Aug 31. Auris Nasus Larynx. 2018. PMID: 28844607 Review.
Cited by
-
Optimal Deep Learning-Based Vocal Fold Disorder Detection and Classification Model on High-Speed Video Endoscopy.J Healthc Eng. 2022 Oct 17;2022:4248938. doi: 10.1155/2022/4248938. eCollection 2022. J Healthc Eng. 2022. PMID: 36353680 Free PMC article.
-
New developments in the application of artificial intelligence to laryngology.Curr Opin Otolaryngol Head Neck Surg. 2024 Dec 1;32(6):391-397. doi: 10.1097/MOO.0000000000000999. Epub 2024 Jul 24. Curr Opin Otolaryngol Head Neck Surg. 2024. PMID: 39146248 Review.
-
Voice disorder recognition using machine learning: a scoping review protocol.BMJ Open. 2024 Feb 24;14(2):e076998. doi: 10.1136/bmjopen-2023-076998. BMJ Open. 2024. PMID: 38401896 Free PMC article.
-
Exploring the Role of Artificial Intelligence Chatbots in Preoperative Counseling for Head and Neck Cancer Surgery.Laryngoscope. 2024 Jun;134(6):2757-2761. doi: 10.1002/lary.31243. Epub 2023 Dec 21. Laryngoscope. 2024. PMID: 38126511 Free PMC article.
-
Severity Classification Using Dynamic Time Warping-Based Voice Biomarkers for Patients With COVID-19: Feasibility Cross-Sectional Study.JMIR Biomed Eng. 2023 Nov 6;8:e50924. doi: 10.2196/50924. eCollection 2023. JMIR Biomed Eng. 2023. PMID: 37982072 Free PMC article.
References
-
- Stachler RJ, Francis DO, Schwartz SR, Damask CC, Digoy GP, Krouse HJ, McCoy SJ, Ouellette DR, Patel RR, Reavis CCW, Smith LJ, Smith M, Strode SW, Woo P, Nnacheta LC. Clinical Practice Guideline: Hoarseness (Dysphonia) (Update) Otolaryngol Head Neck Surg. 2018 Mar;158(1_suppl):S1–S42. doi: 10.1177/0194599817751030. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
