

Progression and Regression of Chronic Kidney Disease by Age Among Adults in a Population-Based Cohort in Alberta, Canada
- PMID: 34100938
- PMCID: PMC8188272
- DOI: 10.1001/jamanetworkopen.2021.12828
Progression and Regression of Chronic Kidney Disease by Age Among Adults in a Population-Based Cohort in Alberta, Canada
Abstract
Importance: The burden of chronic kidney disease (CKD) is expected to increase worldwide as the global population ages, potentially increasing the demand for nephrology services. Understanding whether CKD inevitably progresses or may regress can inform clinical decision-making and health policy.
Objective: To study CKD progression and regression by age in adults with CKD.
Design, setting, and participants: This population-based cohort study used linked administrative and laboratory data to assess adults in the province of Alberta, Canada, with incident mild, moderate, or severe CKD, defined by estimated glomerular filtration rate (eGFR) of 45 to 59, 30 to 44, or 15 to 29 mL/min/1.73 m2 for longer than 3 months, from April 1, 2009, to March 31, 2015. Data were analyzed from July 20 to November 30, 2020.
Exposures: Age.
Main outcomes and measures: Time to the earliest of CKD regression or progression (defined as sustained increase or drop in eGFR category for >3 months, respectively, and a ≥25% increase or decrease in eGFR from baseline, respectively), kidney failure (the earlier of kidney replacement initiation or eGFR <15 mL/min/1.73 m2 for >3 months), death, or censoring (outmigration, 5 years of follow-up, or end of study on March 31, 2017).
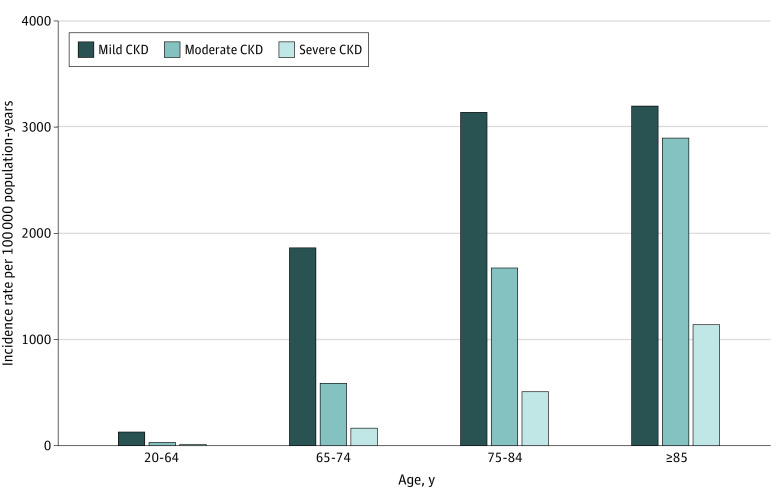
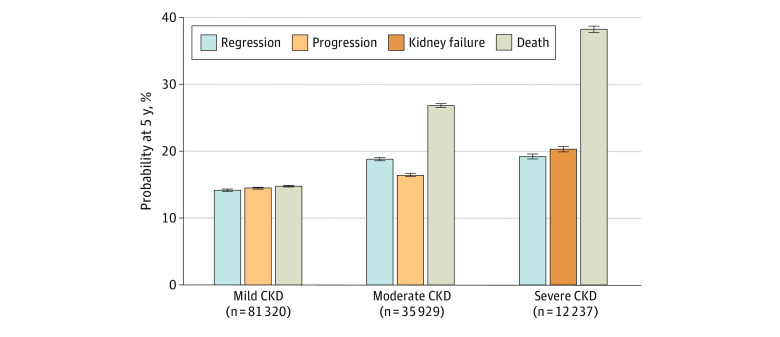
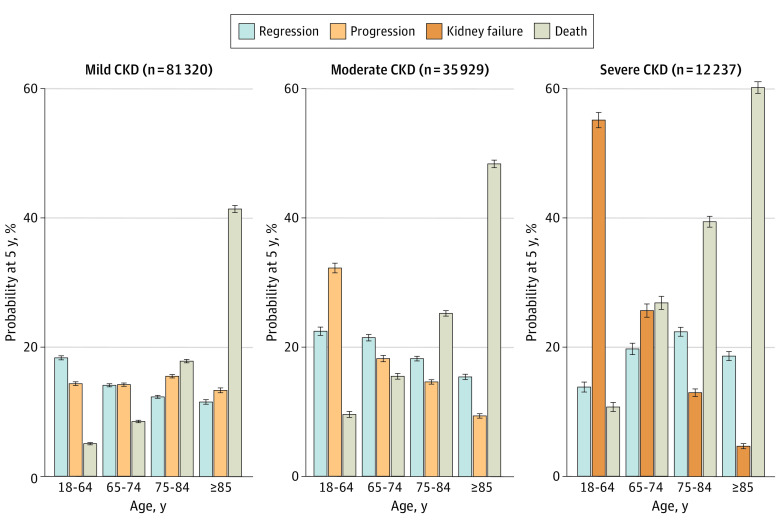
Results: Study participants with CKD (55.2% women and 44.8% men) included 81 320 with mild CKD (mean [SD] age, 72.4 [11.3] years), 35 929 with moderate CKD (mean [SD] age, 77.1 [11.5] years), and 12 237 with severe CKD (mean [SD] age, 76.6 [13.8] years). The annual incidence of CKD increased with advancing age, from 180 per 100 000 population younger than 65 years to 7250 per 100 000 in those 85 years or older. After cohort entry, the 5-year probability of regression was similar to that of progression or kidney failure in mild (14.3% vs 14.6%), moderate (18.9% vs 16.5%), and severe (19.3% vs 20.4%) CKD. As mortality at 5 years increased with advancing age in moderate (from 9.6% for age <65 years to 48.4% for age ≥85 years) and severe (from 10.8% for age <65 years to 60.2% for age ≥85 years) CKD, the risk of progression or kidney failure decreased substantially (for moderate CKD, from 32.3% for <65 years to 9.4% for ≥85 years; for severe CKD, from 55.2% for <65 years to 4.7% for ≥85 years), whereas the probabilities of regression varied to a lesser extent (for moderate CKD, from 22.5% for <65 years to 15.4% for ≥85 years; for severe CKD, from 13.9% for <65 years to 18.7% for ≥85 years).
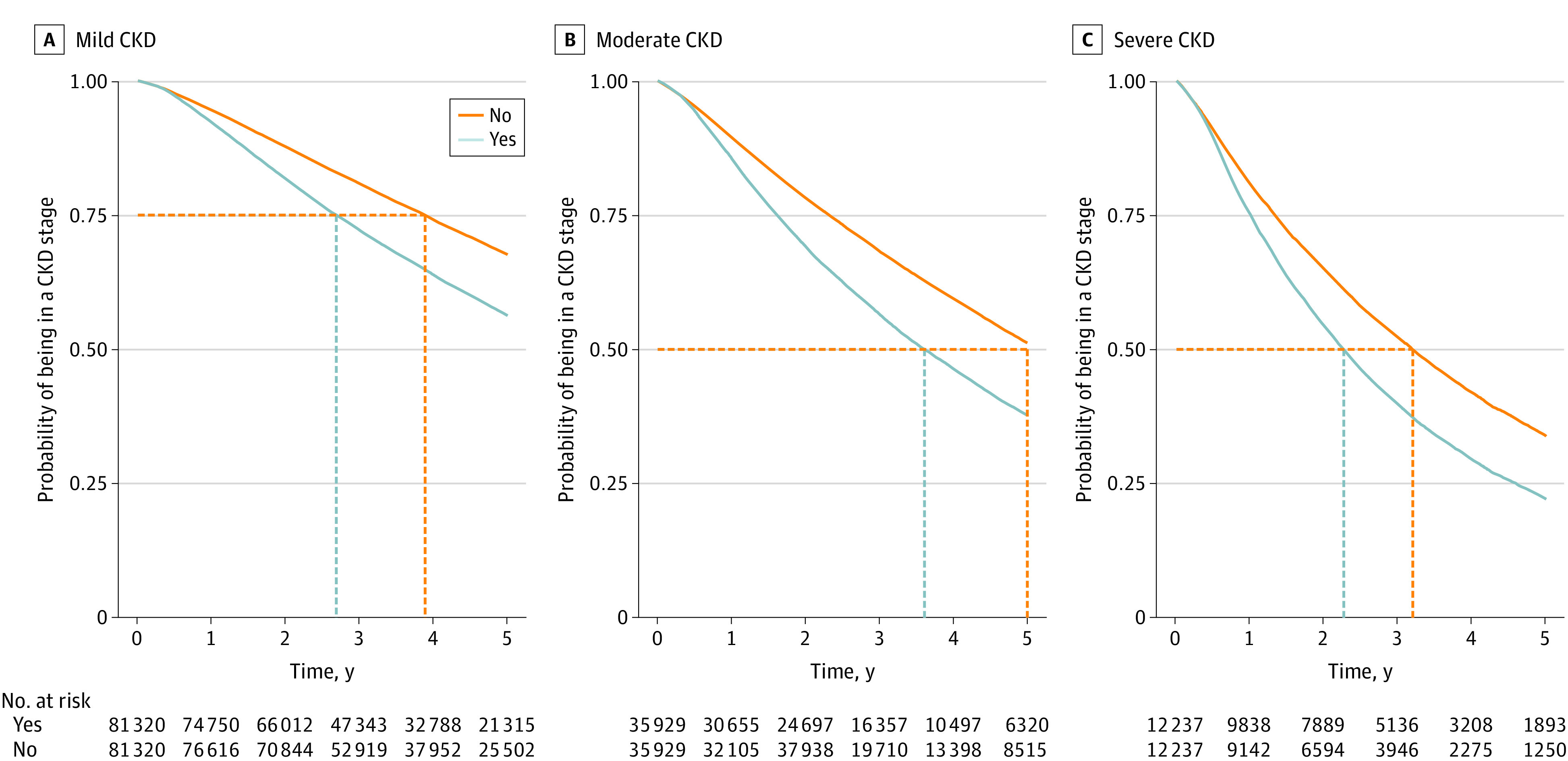
Conclusions and relevance: This cohort study found that with advancing age, CKD regression and death were more likely than CKD progression or kidney failure. These findings have important implications for patient care and for assessing the potential effect of population aging on the burden of CKD.
Conflict of interest statement
Figures
References
-
- United Nations, Department of Economic and Social Affairs, Population Division . World Population Ageing 2019. Published December 31, 2019. Accessed October 25, 2020. https://www.un.org/en/development/desa/population/publications/pdf/agein...
-
- Gansevoort RT, Matsushita K, van der Velde M, et al. ; Chronic Kidney Disease Prognosis Consortium . Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes: a collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011;80(1):93-104. doi:10.1038/ki.2010.531 - DOI - PMC - PubMed
-
- Matsushita K, van der Velde M, Astor BC, et al. ; Chronic Kidney Disease Prognosis Consortium . Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073-2081. doi:10.1016/S0140-6736(10)60674-5 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
