

Hospital-at-Home Interventions vs In-Hospital Stay for Patients With Chronic Disease Who Present to the Emergency Department: A Systematic Review and Meta-analysis
- PMID: 34100939
- PMCID: PMC8188269
- DOI: 10.1001/jamanetworkopen.2021.11568
Hospital-at-Home Interventions vs In-Hospital Stay for Patients With Chronic Disease Who Present to the Emergency Department: A Systematic Review and Meta-analysis
Abstract
Importance: Hospitalizations are costly and may lead to adverse events; hospital-at-home interventions could be a substitute for in-hospital stays, particularly for patients with chronic diseases who use health services more than other patients. Despite showing promising results, heterogeneity in past systematic reviews remains high.
Objective: To systematically review and assess the association between patient outcomes and hospital-at-home interventions as a substitute for in-hospital stay for community-dwelling patients with a chronic disease who present to the emergency department and are offered at least 1 home visit from a nurse and/or physician.
Data sources: Databases were searched from date of inception to March 4, 2019. The databases were Ovid MEDLINE, Ovid Embase, Ovid PsycINFO, CINAHL, Health Technology Assessment, the Cochrane Library, OVID Allied and Complementary Medicine Database, the World Health Organization International Clinical Trials Registry Platform, and ClinicalTrials.gov.
Study selection: Randomized clinical trials in which the experimental group received hospital-at-home interventions and the control group received the usual in-hospital care. Patients were 18 years or older with a chronic disease who presented to the emergency department and received home visits from a nurse or physician.
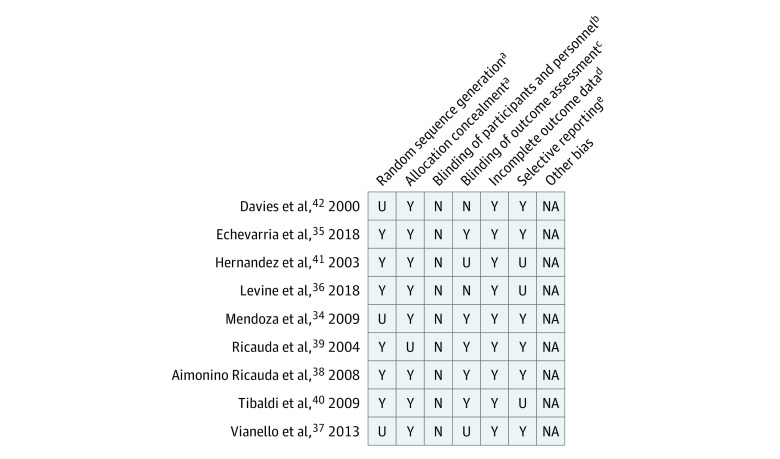
Data extraction and synthesis: Risk of bias was assessed, and a meta-analysis was conducted for outcomes that were reported by at least 2 studies using comparable measures. Risk ratios (RRs) were reported for binary outcomes and mean differences for continuous outcomes. Narrative synthesis was performed for other outcomes.
Main outcomes and measures: Outcomes of interest were patient outcomes, which included mortality, long-term care admission, readmission, length of treatment, out-of-pocket costs, depression and anxiety, quality of life, patient satisfaction, caregiver stress, cognitive status, nutrition, morbidity due to hospitalization, functional status, and neurological deficits.
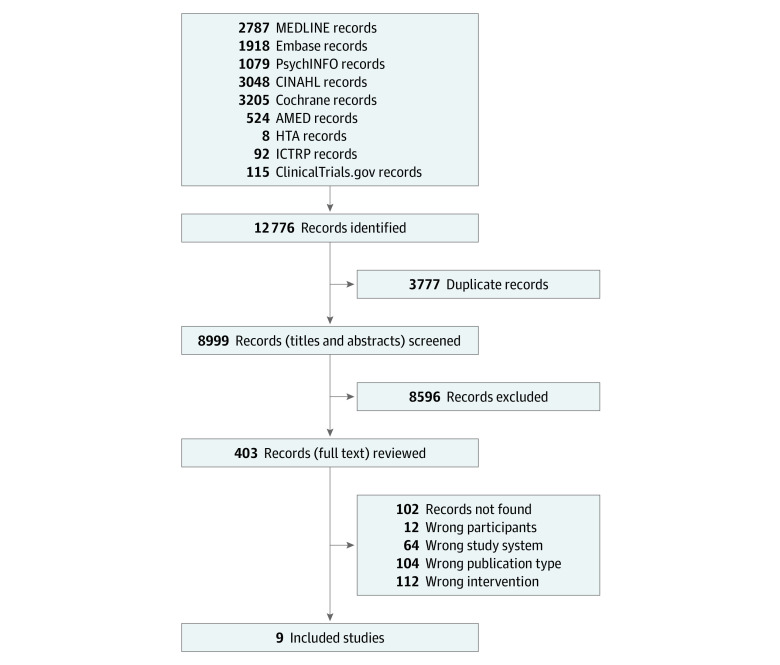
Results: Nine studies were included, providing data on 959 participants (median age, 71.0 years [interquartile range, 70.0-79.9 years]; 613 men [63.9%]; 346 women [36.1%]). Mortality did not differ between the hospital-at-home and the in-hospital care groups (RR, 0.84; 95% CI, 0.61-1.15; I2 = 0%). Risk of readmission was lower (RR, 0.74; 95% CI, 0.57-0.95; I2 = 31%) and length of treatment was longer in the hospital-at-home group than in the in-hospital group (mean difference, 5.45 days; 95% CI, 1.91-8.97 days; I2 = 87%). In addition, the hospital-at-home group had a lower risk of long-term care admission than the in-hospital care group (RR, 0.16; 95% CI, 0.03-0.74; I2 = 0%). Patients who received hospital-at-home interventions had lower depression and anxiety than those who remained in-hospital, but there was no difference in functional status. Other patient outcomes showed mixed results.
Conclusions and relevance: The results of this systematic review and meta-analysis suggest that hospital-at-home interventions represent a viable substitute to an in-hospital stay for patients with chronic diseases who present to the emergency department and who have at least 1 visit from a nurse or physician. Although the heterogeneity of the findings remained high for some outcomes, particularly for length of treatment, the heterogeneity of this study was comparable to that of past reviews and further explored.
Conflict of interest statement
Figures
Comment in
-
Hospitalization at Home for Patients With Acute Exacerbation of Chronic Disease-Further Evidence to Inform Practice.JAMA Netw Open. 2021 Jun 1;4(6):e2111680. doi: 10.1001/jamanetworkopen.2021.11680. JAMA Netw Open. 2021. PMID: 34100941 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
