

Impaired humoral and cellular immunity after SARS-CoV-2 BNT162b2 (tozinameran) prime-boost vaccination in kidney transplant recipients
- PMID: 34101623
- PMCID: PMC8279581
- DOI: 10.1172/JCI150175
Impaired humoral and cellular immunity after SARS-CoV-2 BNT162b2 (tozinameran) prime-boost vaccination in kidney transplant recipients
Abstract
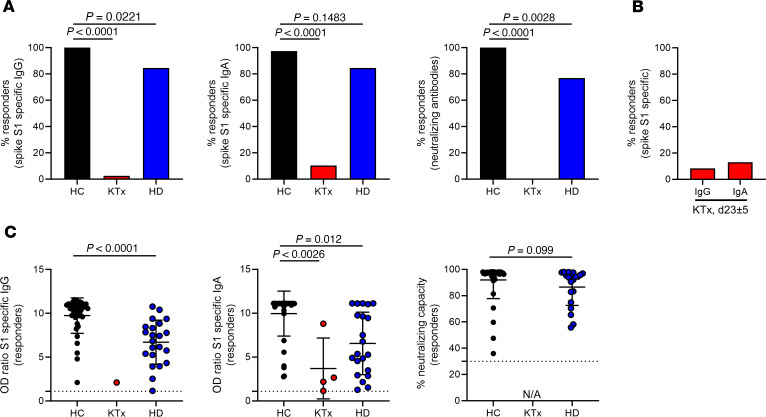
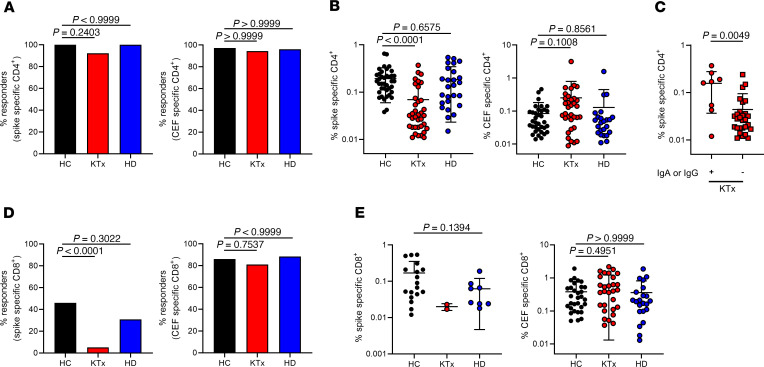
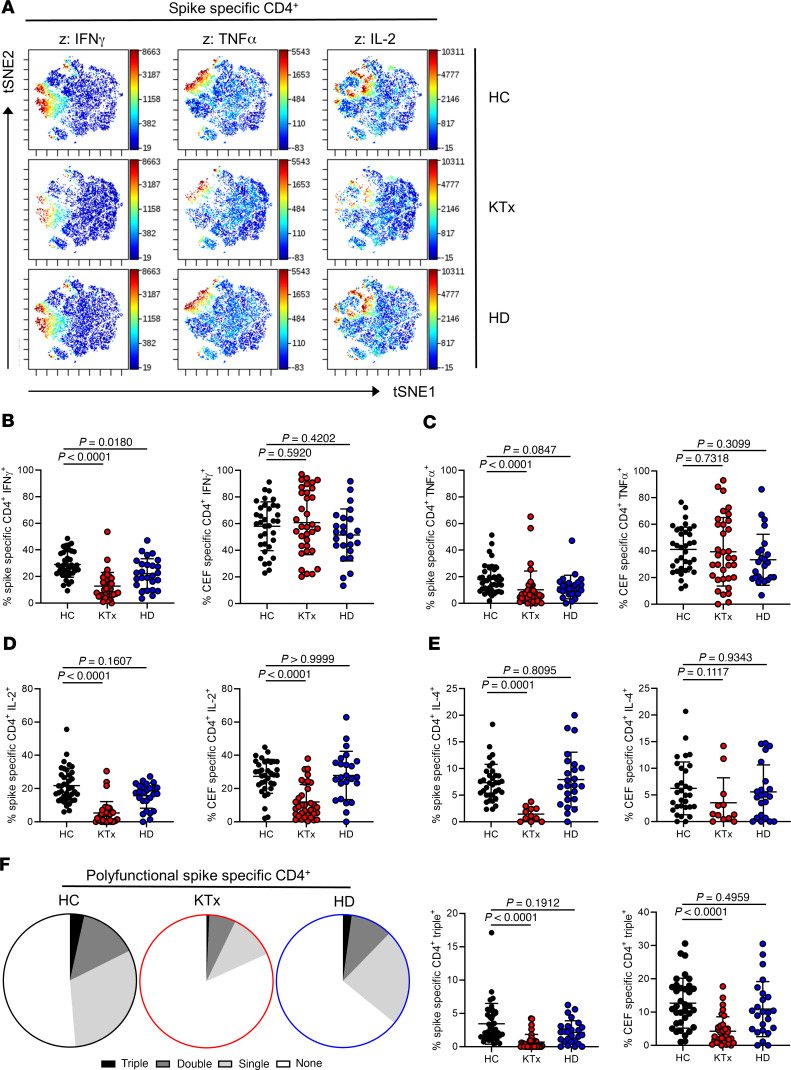
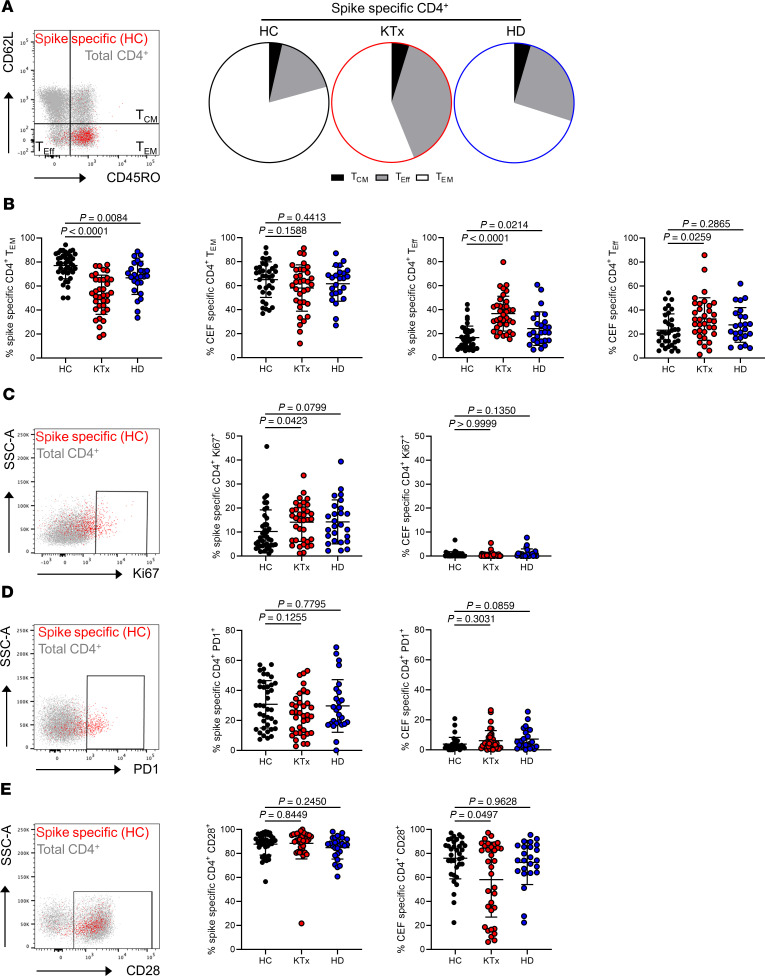
Novel mRNA-based vaccines have been proven to be powerful tools in combating the global pandemic caused by SARS-CoV-2, with BNT162b2 (trade name: Comirnaty) efficiently protecting individuals from COVID-19 across a broad age range. Still, it remains largely unknown how renal insufficiency and immunosuppressive medication affect development of vaccine-induced immunity. We therefore comprehensively analyzed humoral and cellular responses in kidney transplant recipients after the standard second vaccination dose. As opposed to all healthy vaccinees and the majority of hemodialysis patients, only 4 of 39 and 1 of 39 transplanted individuals showed IgA and IgG seroconversion at day 8 ± 1 after booster immunization, with minor changes until day 23 ± 5, respectively. Although most transplanted patients mounted spike-specific T helper cell responses, frequencies were significantly reduced compared with those in controls and dialysis patients and this was accompanied by a broad impairment in effector cytokine production, memory differentiation, and activation-related signatures. Spike-specific CD8+ T cell responses were less abundant than their CD4+ counterparts in healthy controls and hemodialysis patients and almost undetectable in transplant patients. Promotion of anti-HLA antibodies or acute rejection was not detected after vaccination. In summary, our data strongly suggest revised vaccination approaches in immunosuppressed patients, including individual immune monitoring for protection of this vulnerable group at risk of developing severe COVID-19.
Keywords: Adaptive immunity; Immunology; Organ transplantation; T cells; Transplantation.
Conflict of interest statement
Figures
Comment in
-
Interpreting and addressing suboptimal immune responses after COVID-19 vaccination in solid-organ transplant recipients.J Clin Invest. 2021 Jul 15;131(14):e151178. doi: 10.1172/JCI151178. J Clin Invest. 2021. PMID: 34143755 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
