

Characterization of ABH-subtype donor-specific antibodies in ABO-A-incompatible kidney transplantation
- PMID: 34101982
- PMCID: PMC8597088
- DOI: 10.1111/ajt.16712
Characterization of ABH-subtype donor-specific antibodies in ABO-A-incompatible kidney transplantation
Abstract
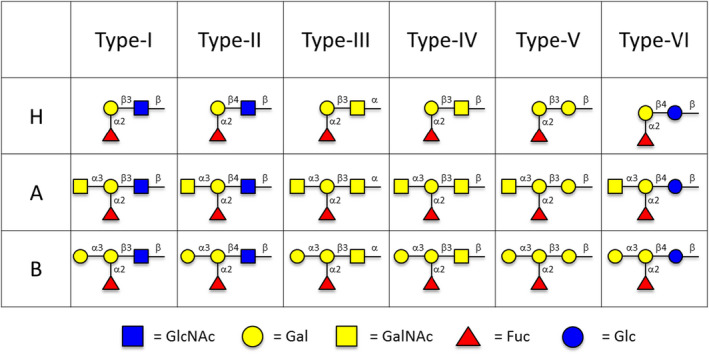
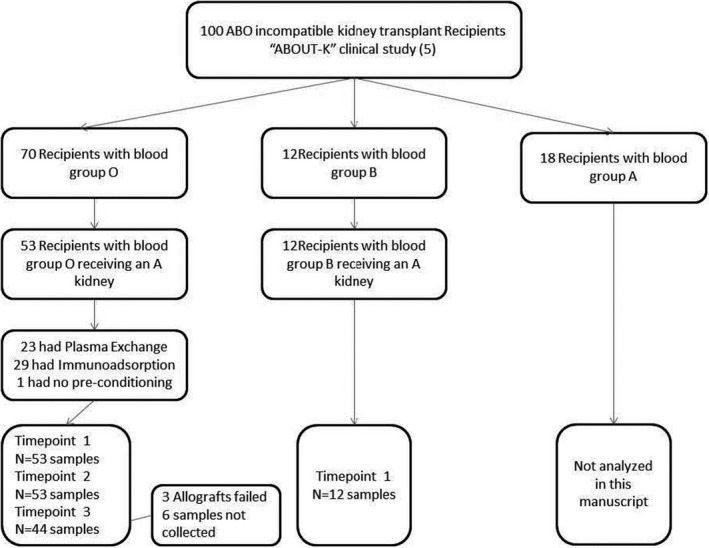
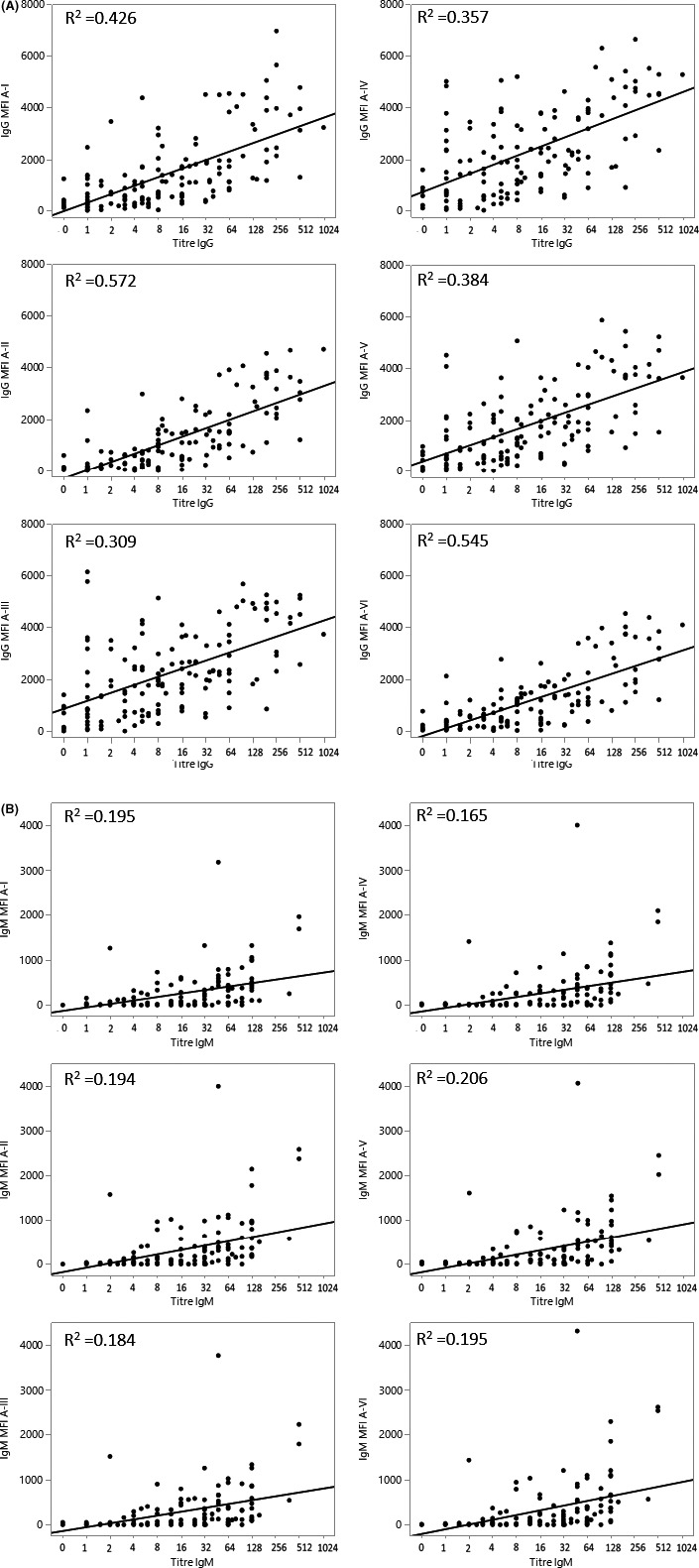
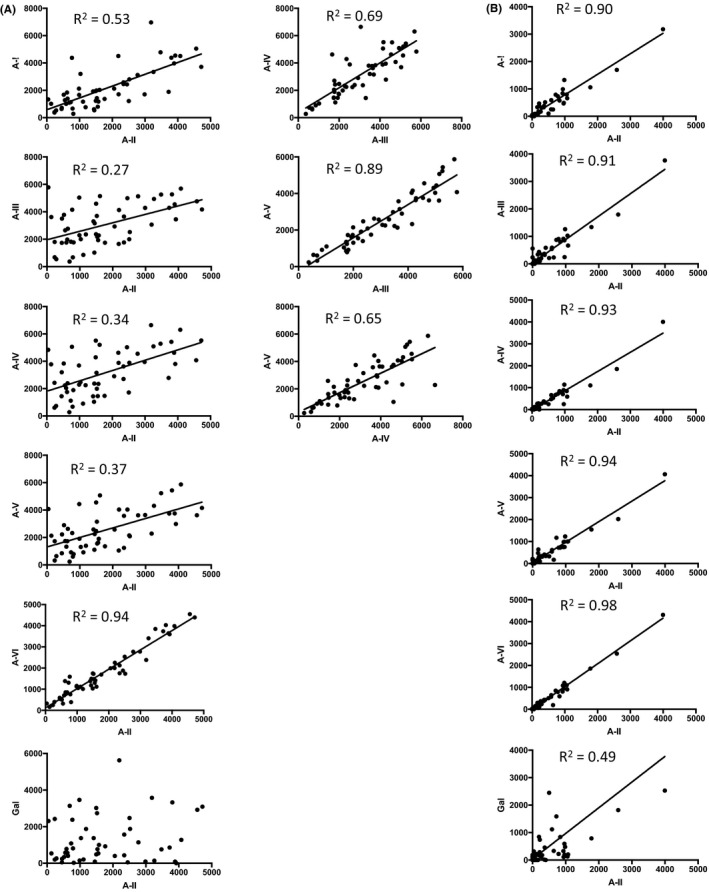
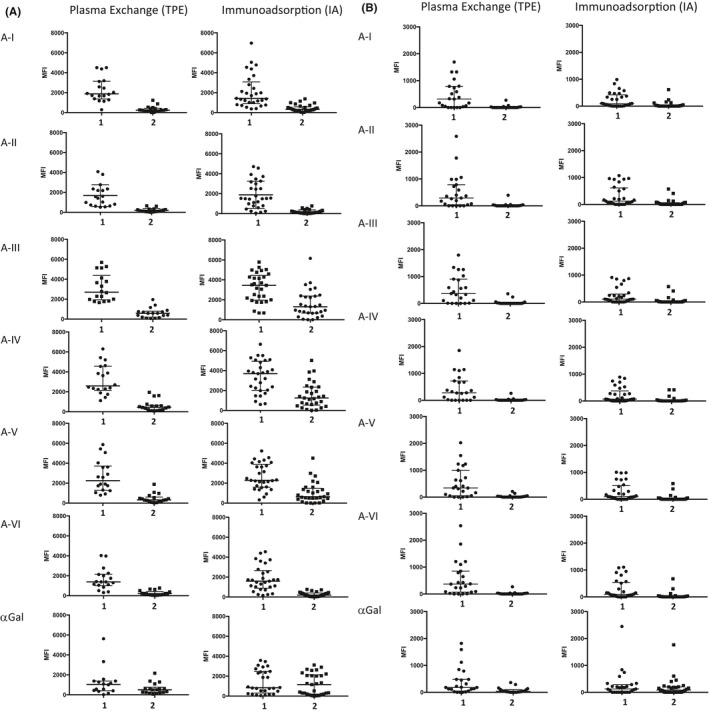
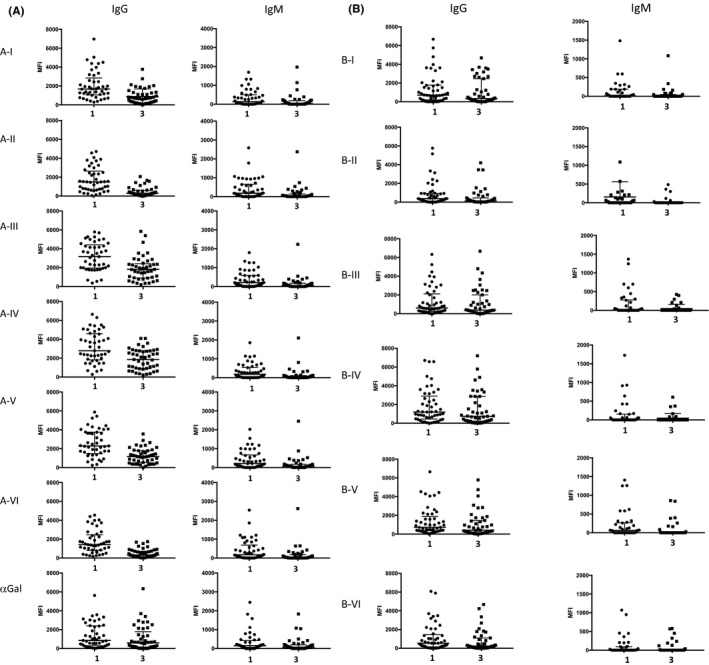
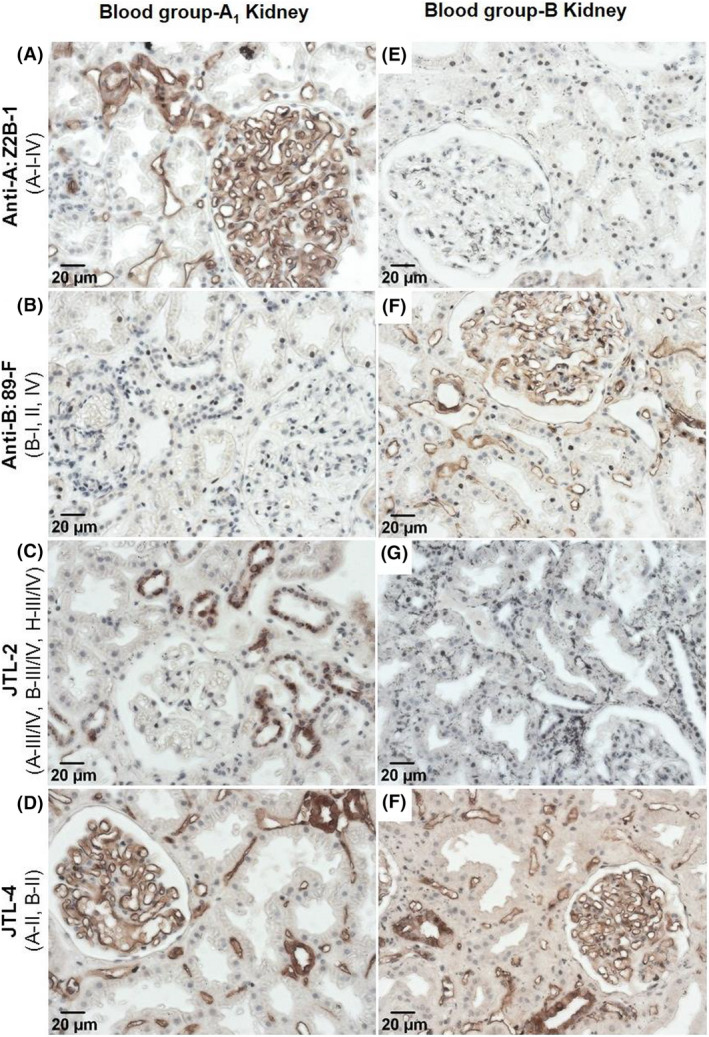
ABO-incompatible (ABOi) transplantation requires preemptive antibody reduction; however, the relationship between antibody-mediated rejection (AMR) and ABO-antibodies, quantified by hemagglutination (HA), is inconsistent, possibly reflecting variable graft resistance to AMR or HA assay limitations. Using an ABH-glycan microarray, we quantified ABO-A antigen-subtype (A-subtype)-specific IgM and IgG in 53 ABO-O recipients of ABO-A kidneys, before and after antibody removal (therapeutic plasma exchange [TPE] or ABO-A-trisaccharide immunoadsorption [IA]) and 1-year posttransplant. IgM binding to all A-subtypes correlated highly (R2 ≥ .90) and A-subtype antibody specificities was reduced equally by IA versus TPE. IgG binding to the A-subtypes (II-IV) expressed in kidney correlated poorly (.27 ≤ R2 ≤ .69). Reduction of IgG specific to A-subtype-II was equivalent for IA and TPE, whereas IgG specific to A-subtypes-III/IV was not as greatly reduced by IA (p < .005). One-year posttransplant, IgG specific to A-II remained the most reduced antibody. Immunostaining revealed only A-II on vascular endothelium but A-subtypes II-III/IV on tubular epithelium. These results show that ABO-A-trisaccharide is sufficient for IgM binding to all A-subtypes; this is true for IgG binding to A-II, but not subtypes-III/IV, which exhibits varying degrees of specificity. We identify A-II as the major, but importantly not the sole, antigen relevant to treatment and immune modulation in adult ABO-A-incompatible kidney transplantation.
Keywords: ABO incompatibility; antibody biology; antigen biology; clinical research/practice; glycomics; histocompatibility; kidney transplantation/nephrology; translational research/science.
© 2021 The Authors. American Journal of Transplantation published by Wiley Periodicals LLC on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
References
-
- Massie AB, Orandi BJ, Waldram MM, et al. Impact of ABO‐incompatible living donor kidney transplantation on patient survival. Am J Kidney Dis. 2020;76:616‐623. - PubMed
-
- de Weerd AE , van Agteren M , Leebeek FW, Ijzermans JN, Weimar W, Betjes MG. ABO‐incompatible kidney transplant recipients have a higher bleeding risk after antigen‐specific immunoadsorption. Transpl Int. 2015;28:25‐33. - PubMed
-
- Becker LE, Siebert D, Susal C, et al. Outcomes following ABO‐Incompatible kidney transplantation performed after desensitization by nonantigen‐specific immunoadsorption. Transplant. 2015;99:2364‐2371. - PubMed
-
- Bentall A, R. Barnett AN, Braitch M, et al. Clinical outcomes with ABO antibody titer variability in a multicenter study of ABO‐incompatible kidney transplantation in the United Kingdom. Transfusion. 2016;56:2668‐2679. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
