

Prognosis of variceal and non-variceal upper gastrointestinal bleeding in already hospitalised patients: Results from a French prospective cohort
- PMID: 34102016
- PMCID: PMC8280797
- DOI: 10.1002/ueg2.12096
Prognosis of variceal and non-variceal upper gastrointestinal bleeding in already hospitalised patients: Results from a French prospective cohort
Abstract
Objectives: Patients who develop upper gastrointestinal bleeding (UGIB) while in hospital appear to have a poor prognosis. Our study aims at analysing the difference in outcome between in-patients (IPs) and out-patients presenting with variceal and non-variceal UGIB.
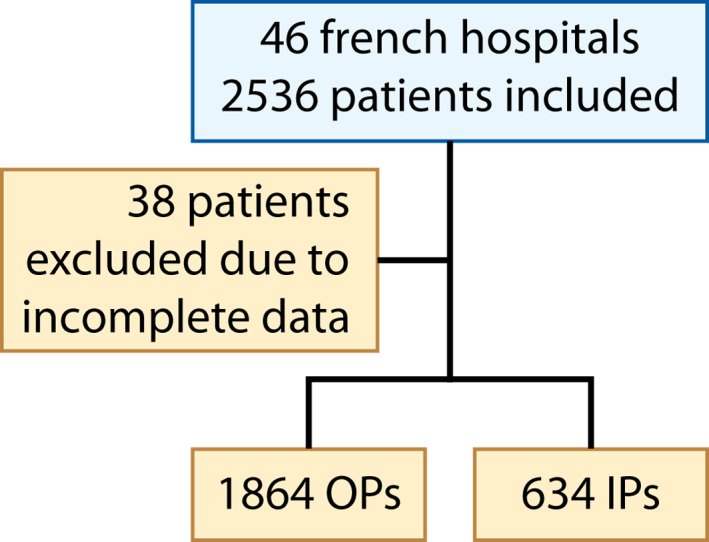
Methods: We conducted a multicentre prospective study by collecting data about variceal and non-variceal UGIB cases through 46 hospitals in France between November 2017 and October 2018. We then compared baseline demographic features, endoscopic findings and outcome between patients who developed variceal and non-variceal UGIB on admission (OPs) and those at least 24 h after hospitalisation (IPs). Our primary end-point was mortality and re-bleeding rates at 6 weeks of bleeding onset.
Results: A total of 2498 UGIB cases were identified, of whom 634 (25.4%) occurred in IPs. IPs were older than OPs (72.5 vs. 67.2 years old, p < 0.001) and had a higher rate of comorbidities (38.9% vs. 26.6%, p < 0.0001). Their bleeding was more severe with a Rockall score of >5 present in 40.9% (vs. 30.3% in OPs, p < 0.0001). The 6-week mortality rate was significantly higher in IPs when compared to OPs (21.7% vs. 8%, p < 0.0001). Prothrombin time <50% and rebleeding were the only independent predictors of mortality (p = 0.001 and 0.003, respectively). Six-week rebleeding occurred more frequently among IPs (18.6% vs. 14.4%, p = 0.015) and predictors included female sex, active bleeding upon endoscopy and a Blatchford score >11 (p = 0.017, 0.011 and 0.008, respectively).
Conclusion: IPs who develop variceal and non-variceal UGIB are more likely to be elderly with more comorbidities. They have a higher rate of mortality and rebleeding. Independent predictors of mortality were underlying coagulopathy and bleeding recurrence. An optimal bleeding management and efficient rebleeding prevention may improve outcome in these patients.
Keywords: gastrointestinal bleeding; in-patients; non-variceal bleeding; peptic ulcer disease; portal hypertension; upper GI bleeding; upper GI endoscopy; variceal bleeding.
© 2021 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC. on behalf of United European Gastroenterology.
References
-
- Leerdam ME, Vreeburg EM, Rauws EAJ, Geraedts AAM, Tijssen JGP, Reitsma JB, et al. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol. 2003;98(7):1494–9. - PubMed
-
- Theocharis GJ, Thomopoulos KC, Sakellaropoulos G, Katsakoulis E, Nikolopoulou V. Changing trends in the epidemiology and clinical outcome of acute upper gastrointestinal bleeding in a defined geographical area in Greece: J Clin Gastroenterol. 2008;42(2):128–33. - PubMed
-
- Jamal MM, Samarasena JB, Hashemzadeh M, Vega KJ. Declining hospitalization rate of esophageal variceal bleeding in the United States. Clin Gastroenterol Hepatol. 2008;6(6):689–95. - PubMed
-
- Nahon S, Hagège H, Latrive J, Rosa I, Nalet B, Bour B, et al. Epidemiological and prognostic factors involved in upper gastrointestinal bleeding: results of a French prospective multicenter study. Endoscopy. 2012;44(11):998–1008. - PubMed
-
- Jairath V, Thompson J, Kahan BC, Daniel R, Hearnshaw SA, Travis SPL, et al. Poor outcomes in hospitalized patients with gastrointestinal bleeding: impact of baseline risk, bleeding severity, and process of care. Am J Gastroenterol. 2014;109(10):1603–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
