

Sacubitril-valsartan initiation in chronic heart failure patients impacts sleep apnea: the ENTRESTO-SAS study
- PMID: 34102018
- PMCID: PMC8318447
- DOI: 10.1002/ehf2.13455
Sacubitril-valsartan initiation in chronic heart failure patients impacts sleep apnea: the ENTRESTO-SAS study
Abstract
Aims: Optimizing medical cardiac treatment for sleep apnoea (SA) in patients with chronic heart failure and reduced ejection fraction (HFrEF) is an expert Grade C recommendation based on six studies encompassing a total of 67 patients only. Whether sacubitril-valsartan (SV), a cornerstone of HFrEF medical treatment, impacts SA is unknown and requires evaluation.
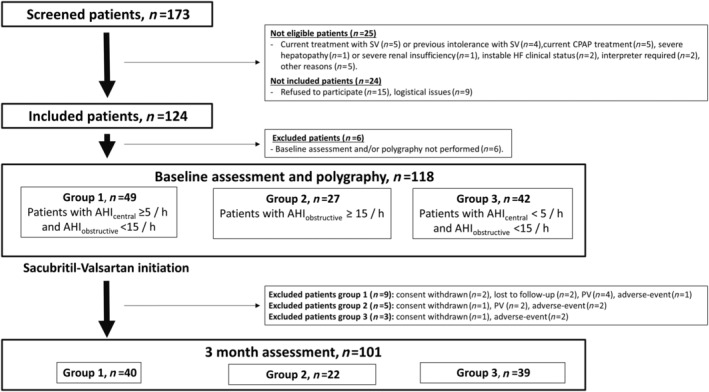
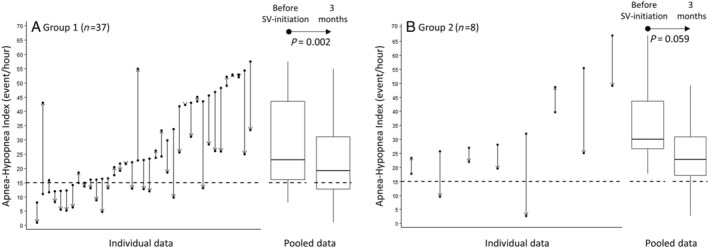
Methods and results: The ENTRESTO-SAS trial is a six-centre, prospective, open-label real-life cohort study (NCT02916160). Ambulatory patients eligible for SV (i.e. HFrEF adults who remain symptomatic despite optimal treatment) were evaluated before and after 3 months of SV (including nocturnal ventilatory polygraphy); 118 patients were final analysed [median age was 66 (IQ25-75 : 56-73) years, 81.4% male, 36.5% New York Heart Association III-IV, N-terminal pro-B-type natriuretic peptide level of 1564 (701-3376) ng/L, left ventricular ejection fraction of 30 (25-34)%, 60.7% ischaemic HFrEF, 97.5% initially treated with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, 83.9% with beta-blockers, 64.4% with mineralocorticoid receptor antagonists, and 74.6% with diuretics]. Three groups were defined according to initial central/obstructive apnoea-hypopnoea indices (AHIs): G1 (n = 49, AHIcentral ≥ 5/h and AHIobstructive < 15/h); G2 (n = 27, AHIobstructive ≥ 15/h); and G3 (n = 42, AHIcentral < 5/h and AHIobstructive < 15/h). At 3 months, the AHI (main predefined outcome) decreased significantly by -7.10/h (IQ25-75 : -16.10 to 0.40; P < 0.001) in G1 + G2 without positive airway pressure treatment (45 patients, median initial AHI of 24.20 (IQ25-75 : 16.40-43.50)/h). Of these, 24.4% presented an AHI decrease ≥50% and 37.78% had a final AHI < 15/h (tendency for improvement from an initial value of 20%: P = 0.0574). For G1 patients (n = 37), AHI significantly decreased from a median of 22.90 (16.00-43.50)/h to 19.20 (12.70-31.10)/h (P = 0.002). For G2 patients (n = 8), AHI decreased from a median of 30.10 (26.40-47.60)/h to 22.75 (14.60-36.90)/h (statistically non-significant, P = 0.059).
Conclusions: In this real-life population, SV treatment for 3 months in SA patients is associated with a significant decrease in AHI. These results support the current guidelines that recommend first an optimization of the HFrEF treatment in patients with HFrEF and central SA. A potential positive airway pressure sparing effect merits further investigation.
Keywords: Continuous positive airway pressure; Heart failure; Sacubitril-valsartan; Sleep apnoea; Sleep-disordered breathing.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
D.J. reports personal fees from Philips Healthcare, ResMed, GSK, Boehringer Ingelheim, AstraZeneca, Chiesi Farmaceutici, Sanofi, Novartis, and Bastide Le Confort Médical; personal fees and non‐financial support from SEFAM; grants, personal fees, and non‐financial support from Lowenstein and Nomics; grants and personal fees from APARD; and grants from ADENE, outside the submitted work. P.B. reports personal fees from Novartis, outside the submitted work. M.G. reports personal fees from Novartis, outside the submitted work. P.F. reports personal fees from Novartis and AstraZeneca and non‐financial support from Abbot, outside the submitted work. J.‐E.R. reports personal fees from AstraZeneca, Novartis, and Vifor, outside the submitted work. M.‐P.C. reports non‐financial support from Eole Santé and SOS Oxygène, outside the submitted work. F.P. reports personal fees from Novartis, Pfizer, Actelion, and Vifor, outside the submitted work. J.‐P.M. reports grants from APARD and Novartis, outside the submitted work. C.M.S. reports grants from AstraZeneca, outside the submitted work. N.M. reports personal fees from AstraZeneca and grants from GSK, outside the submitted work. A.B. reports grants, personal fees, non‐financial support, and other from AstraZeneca and Boehringer Ingelheim; grants, personal fees, and other from GSK; personal fees, non‐financial support, and other from Novartis, Chiesi Farmaceutici, and Actelion; personal fees and other from Teva and Regeneron; other from Gilead; and personal fees and non‐financial support from Roche, outside the submitted work. F.R. reports grants from Novartis, during the conduct of the study; grants, personal fees, and non‐financial support from Air Liquide; grants and personal fees from Abbott, Novartis, and AstraZeneca; and personal fees from Vifor, Servier, Abiomed, ZOLL, Medtronic, ResMed, LVL, Eole Santé, Pfizer, Novo Nordisk, Amgen, and Boehringer Ingelheim, outside the submitted work. E.N., M.D., V.P., F.G., and N.P. report no conflicts of interest in relation to the present work.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola V‐P, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, Authors/Task Force Members, Document Reviewers . 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016; 18: 891–975. - PubMed
-
- Stewart S, Ekman I, Ekman T, Odén A, Rosengren A. Population impact of heart failure and the most common forms of cancer: a study of 1 162 309 hospital cases in Sweden (1988 to 2004). Circ Cardiovasc Qual Outcomes 2010; 3: 573–580. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous