

Quality of Life Is Independently Associated With Neurocognitive Function in Patients With Brain Tumors: Analysis of a Prospective Clinical Trial
- PMID: 34102297
- PMCID: PMC8463493
- DOI: 10.1016/j.ijrobp.2021.05.134
Quality of Life Is Independently Associated With Neurocognitive Function in Patients With Brain Tumors: Analysis of a Prospective Clinical Trial
Abstract
Purpose: We conducted the first prospective longitudinal study examining the independent association between patient-reported health-related quality of life (hrQoL) (physical, social/family, emotional, functional, and brain cancer-specific) and neurocognitive function (NCF), while controlling for mood symptoms in patients with primary brain tumors.
Methods and materials: Patients with primary brain tumors (n = 59) receiving brain radiation therapy underwent hrQOL (Functional Assessment of Cancer Therapy-Brain), mood (Beck Depression and Anxiety Inventories), and neurocognitive evaluation at baseline and 3, 6, and 12 months postradiation therapy in a prospective clinical trial. Neurocognitive assessments measured attention/processing speed, memory, and executive function, including the Delis-Kaplan Executive Function System Verbal Fluency, Hopkins Verbal Learning Test Revised (HVLT-R), and Brief Visuospatial Memory Test. Subjects underwent neurocognitive, mood, and hrQoL assessments in the same testing session. Multivariable linear mixed-effects models assessed associations between hrQOL and NCF over time, controlling for patient, tumor, and treatment characteristics as well as timepoint-specific patient-reported mood (ie, anxiety and depression symptoms). P values were adjusted for multiple comparisons.
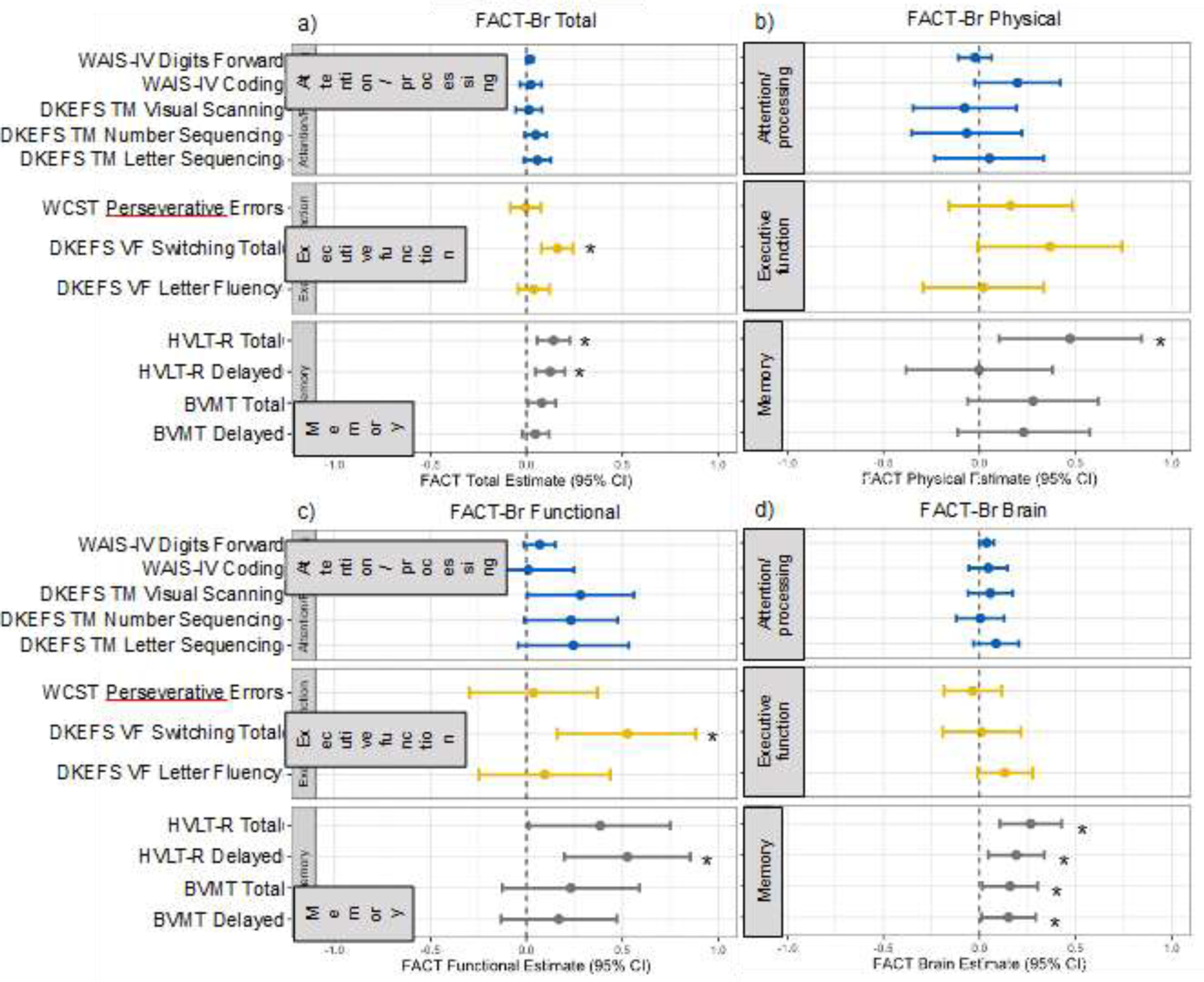
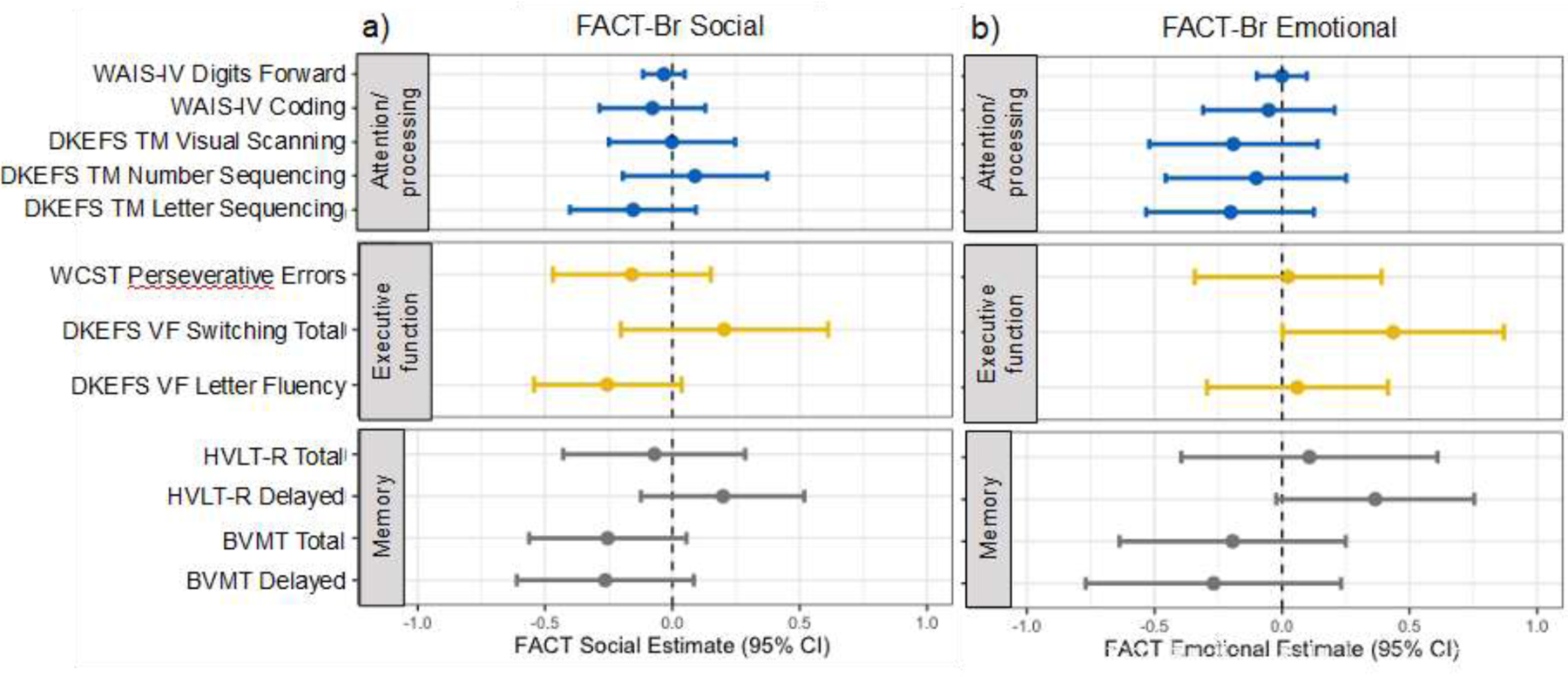
Results: Higher physical hrQoL was associated with better verbal memory (HVLT-R Total Recall, P = .047), and higher functional hrQoL was associated with better executive function (Delis-Kaplan Executive Function System Verbal Fluency Switching Total, P = .009) and verbal memory (HVLT-R Delayed Recall, P = .006). Higher brain tumor-specific hrQoL was associated with better verbal and nonverbal memory (HVLT-R Total, P = .004 and Delayed Recall, P = .030; Brief Visuospatial Memory Test Total, P = .049 and Delayed Recall, P = .049). There was no association between social/family or emotional hrQoL and NCF after controlling for mood.
Conclusions: Higher physical, functional, and brain tumor-specific hrQoL were associated with better executive function and memory among patients with primary brain tumors. Physical and functional impairments are correlated with cognitive performance. Interventions to maximize quality of life after treatment may influence neurocognition and vice versa.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest:
JAH-G reports grant funding from Varian Medical Systems, unrelated to the present study. CRM has research funding from GE Healthcare, unrelated to the current study.
Figures


References
-
- Brown PD, Jaeckle K, Ballman KV., et al.Effect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases a randomized clinical trial. JAMA - J Am Med Assoc 2016;316(4):401–409. doi:10.1001/jama.2016.9839 - DOI - PMC - PubMed
-
- Gilbert MR, Dignam JJ, Armstrong TS, et al.A randomized trial of bevacizumab for newly diagnosed glioblastoma. N Engl J Med 2014;370(8):699–708. 10.1056/NEJMoa1308573\nhttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed12&NEW.... - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
